
Home visits in brain tumor patient: how nurse and family members cooperate in tumor patient’s family self-care
Introduction
Glioma is the most common primary malignant tumor in the central nervous system. It occurs mainly in people aged 30-60 years old. Gliomas are malignant brain tumors and they are classified into WHO grade I-IV. WHO grade I gliomas are low grade brain tumors, while WHO grade IV gliomas are the most malignant brain tumors. Recurrence rate after surgery is high, and the loss of brain function will be obvious during tumor progression, which affecting patients’ life qualities.
Helping patients and their family members to build up healthy behavioral habits and lifestyles is important for meeting their needs for community healthcare services. Home visits enables active involvement of patients and their family members, performance of well-targeted assessment, provision of emotional support, psychological counseling and health education (1). It also strengthens the patients’ self-care ability, awareness of home environment safety and extent of functional rehabilitation, thus the postoperative patients’ quality of life could be improved. As a result, home care and community nursing would become an essential part for delay of disease progression and improvement of patients’ quality of life.
With the changing of medical model, the focus of nursing work has shifted from disease treatment to patient-centered care (2). Provision of comprehensive and all-round service from hospital to hospital patients is essential for satisfying their human health needs (3).
The family shapes each individual and no family exists independently. In society, family certainly plays an important role. Therefore, when nurses are able to evaluate family, they would diagnose the patients and their families appropriately, and take the proper nursing measures (4). Hence nurses are the main professionals who carry out community health education (5). In order to provide excellent nursing service, implement holistic primary nursing, promote individualized health education activities, we launched continuous nursing services by home visits at the Neurosurgery Department of Huashan Hospital, Fudan University, Shanghai. Within one week after discharge from hospital, primary nurses conduct telephone follow-ups or home visits in groups of two. They act as professional advisers to further provide health care for patients. This study illustrates in details how continuous nursing services are carried out in brain tumor patients.
Patient and materials
Family situation
It’s a middle-class family with three members. The husband is 43 years old and healthy. He owned a barber shop in the residential area in the past three years. He is gentle with good workmanship and the business was good. He loves his wife and son. Mrs Wu (the patient in our study) is 46 years old, and works as a nurse in the department of epidemiology at a large hospital for about 20 years. She works hard and is a healthy lady. The son is a student of the junior high school.
It was a fall morning. After finishing a night shift, Mrs Wu fell off her bicycle on the way home. She was sent to the hospital for examination. The head CT scan showed an intracranial tumor, and she was hospitalized for further evaluation and treatment.
Mrs Wu recalled, she heard someone call her, and she turned around, then fell off. She complained she always had the same symptom recently. She was diagnosed of temporal glioma after expert consultation. The neurosurgeon removed the tumor for her, and tumor pathology was glioblastoma multiforme (GBM, WHO IV), which is the most malignant glioma subtype. She received radiotherapy and chemotherapy after surgery. But the tumor was relapsed seven months later, and she underwent second operation. Then her physical condition deteriorated, she suffered from hair loss, paralysis, and vision decrease in recent years. She is now too weak to take care of herself. Thus, her husband closes the barber shop and takes care of her. But the economic burden is too much because of limited family income.
Family housing
They moved to a new apartment in a new residential area in Pudong, Shanghai due to the municipal reconstruction of the old place. The new apartment is on the second floor with simple decoration because of their economic difficulty, and the furniture is old but clean.
There is green coverage with nearby subway and bus stations, and there are no industrial factories around the area. Moreover, there are some supporting facilities such as hospital, car parks and shopping market. Primary and secondary schools and police station are also not far from their home.
Family organization
In the past, family decisions were usually made after member discussion, and Mrs Wu did the housework. But now, Wu’s husband mainly did the family decisions.
The communication between parents and the son was well. Sometimes Mrs Wu may spoil her child. But the boy didn’t have bad friends in the school.
The role of each family member is accepted by others. Before Mrs. Wu was sick, she took care of her son and taught him. Her husband also took the responsibility to play with him and taught him swimming.
Currently, the main focus of the family was Mrs. Wu’s health. Sometimes Mrs. Wu could feel better, which is positive for the whole family’s motivation.
Results
Family function
Criteria for self-care of family members
Air: there is no bad smell both indoors and outdoors. Mrs Wu’s husband is a non-smoker. There is nothing that could affect the air quality. Food: Mrs Wu worked three shifts in the hospital before she was ill, and her husband managed the barber shop himself. Their lunches at workplace were simple snacks. In the evening, they sometimes bought food because their son would have dinner at home. But now her husband buys food and cooks for her, such as chicken soap, special veg meals and non-veg meals. Drinking water: in the past five years, they bought the drinking water and the cost is 14 RMB/barrel of 19 L. The household water is tap water. Family health: the family holds good habits. Mrs Wu goes to the toilet with the help of her husband. The home waste is put into bags and disposed off by residential garbage collection. Activity: Mrs Wu mainly takes activities at home. Sometime she enjoys sunshine in the balcony. They go to hospital by taxi.
To promote the development of family members’ personalities and to meet the members’ psychological and social needs
Alone: Mrs Wu lives in a separate room. After school, her son goes to her room and talks to her. Social interaction: Mrs Wu began to believe in Buddhist and went to temple twice per month after she was ill. Sometimes she asked her husband to go there for her. She said her life was saved by the Buddha. She had little social activities. Personal development for family members: the son knows his mother is sick and his father should take care of his mother. Thus he should study hard by himself. Family relationship: Mrs Wu and her husband lived happy for several years. They have good relationships and they care for each other. But her husband is desperate when she is sick at home. Behavioral control: there were no bad behaviors in the family members (6). If they feel uncomfortable, they will go to hospital in time. Cognitive development: their knowledge was mainly acquired from TV and radio. Sometimes her husband seeks help from the hospital for family healthcare knowledge.
Risk prevention
The real situation of family self-care: there was no accident for the family. Mrs Wu was a nurse, and she used medicine for her own and family members’ disease. Her husband also goes to hospital for routine check-up. Thermos and other dangerous objects are kept in safe places at home and nothing was placed bedside. The situation of preventive health measures: they live on the second floor, so there was a great disturbance of mosquitoes and flies. Last year, they installed screen windows and screen doors in order to avoid the pests. The son received vaccination in school.
The ability of adaptability
Mrs Wu could not accept the sudden attack of the disease at first. She cried when she was admitted for the operation, and even had suicidal thoughts. Her husband even didn’t know what to do at that time. After operation, her colleagues helped her family to get through the hard times.
Health situation and cognition
The family members have insufficient knowledge and skills of taking care of Mrs Wu, and they seek for the support for body movement and skin integrity.
After home visits, we found Mrs. Wu has health problems. Knowledge, skills, motivation and human social factors of the main problems were assessed. The details are as follows: Mrs Wu was anxious about the sudden change of her life. Before surgery, she was beautiful and fashion. Now she is almost blind, hair loss and paralysis. Her husband has no income. The family is only supported by her small incomes (see Table 1). Mrs Wu has impaired physical mobility. Her daily life depends on her husband. If her husband goes out, the risk exists for her. Her skin integrity is impaired. She has to stay in bed because of paralysis. Skin rash sometimes occurs (see Table 2). Moreover, Mrs Wu is suffering from her disability of housekeeping skills. She could not live without her husband. There is insufficient money for house refurbishment. She was worried about her son’s study and health (see Table 3).
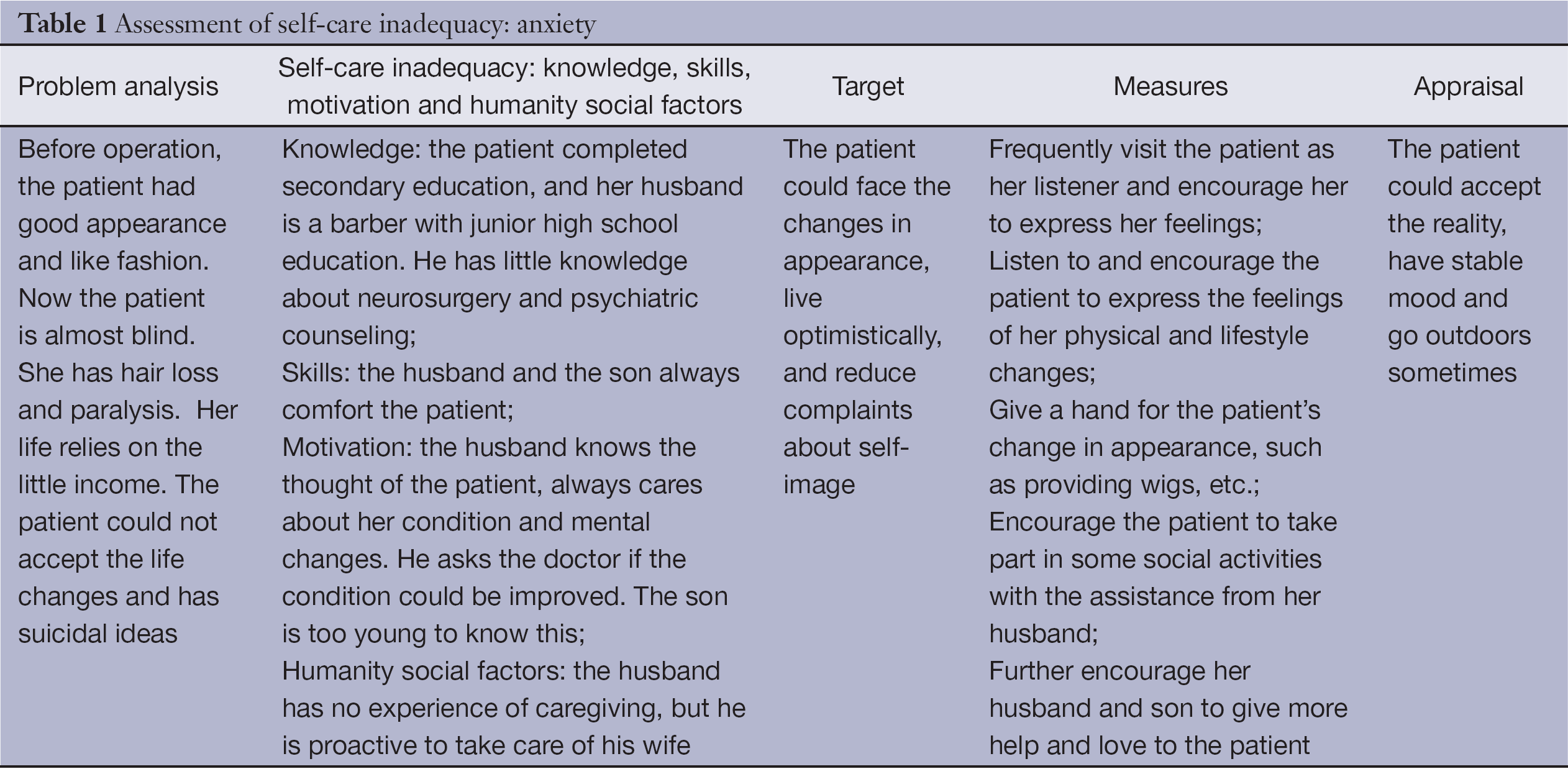
Full table
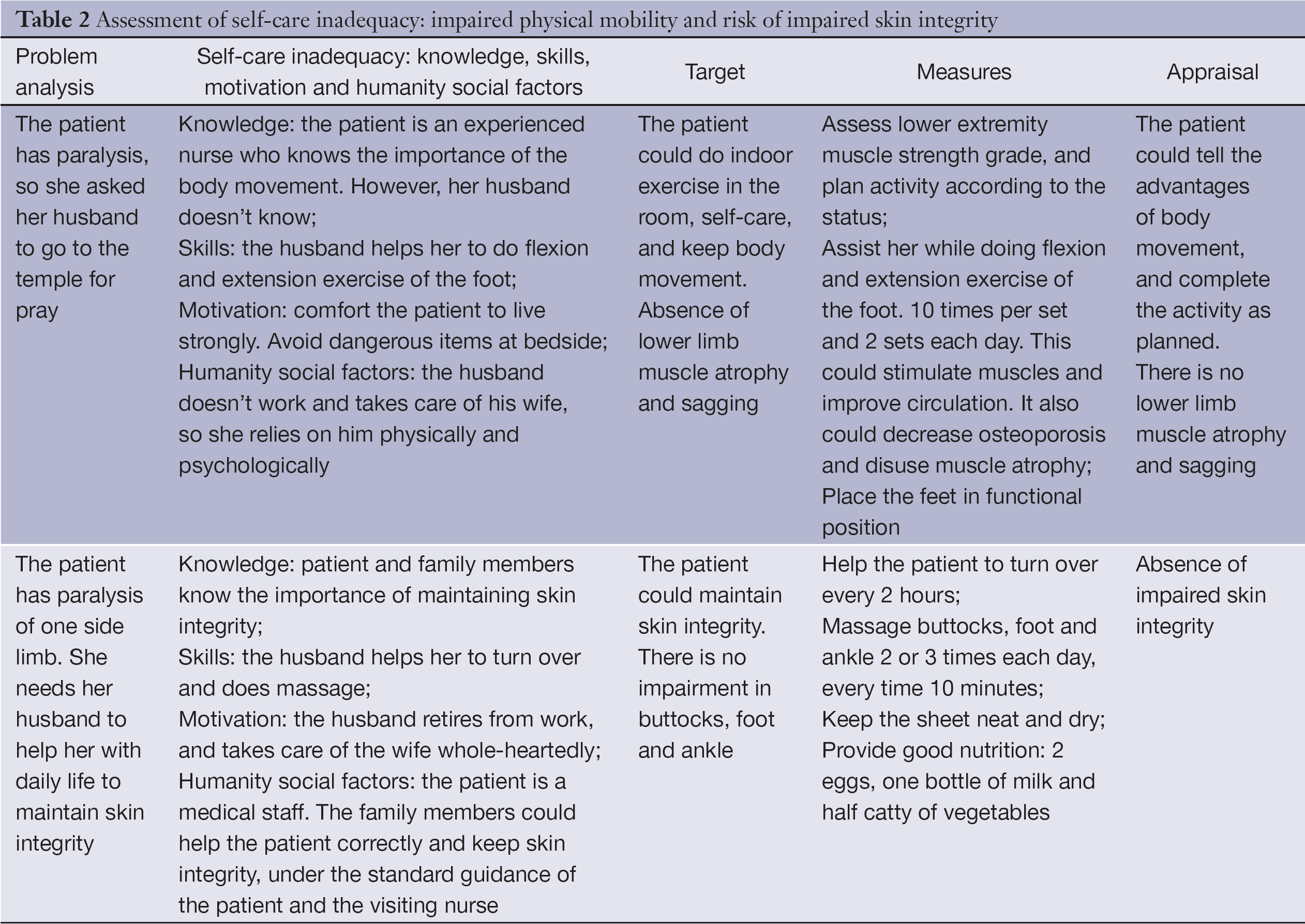
Full table
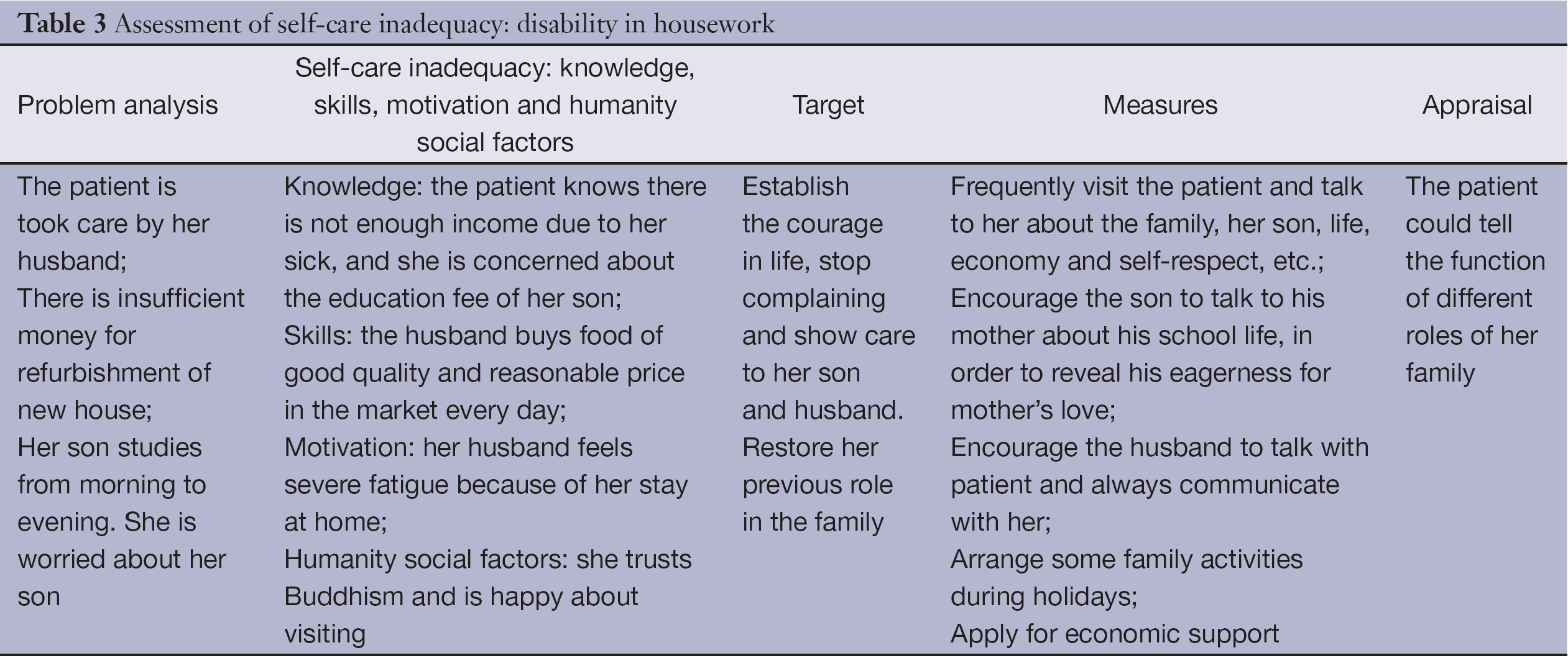
Full table
Evaluation of family self-care and demand
If the patients need some advices, the nurses would provide the information and educate them (7). In this case, the patient could not take care of herself after discharge. She needs help from her family members and community nurses. The nurses could help the family in the following aspects, providing family education and evaluation based on the health problem, shortage of skills and knowledge for caregiving (Tables 1-3). Considering Mrs Wu’s demands and benefits, caregivers of the family may be overburdened. Therefore, every means should be tried to decrease their burdens (8). As a result, with the health education and instructions from the visiting nurses, Mrs Wu and her family showed good progression in their self-care abilities (see Tables 1-3).
Discussion
The holistic nursing care should include health education (9). According to the family health assessment guide, the community nurses should encourage patients to take part in. When assessing the subjects and their families or living environment, nurses should be well-prepared, pay attention to the way of inquire and listen carefully. When evaluating the patient and his family or environment factor, a complete integrated understanding of the health problems of the patient and his family is required. Furthermore, they should look for the potential risk factors among the patient and the family members (10).
Home environment is the place of choice for Chinese to recuperate. Assessment and instruction of home environment safety is essential for the home care of postoperative glioma patients. This not only requires attentions from nurses, but also efforts from their families. During the home visits of this patient, nurses improved the family members’ roles and functions continuously. With cognitive education and behavioral intervention (11), the nurses performed health education and instructions according to the inadequacy of the patient and her family members. The patient’s family members looked after her whole-heartedly. They learned about the skills of repositioning and nursing safety (12), thus the patient could receive standard nursing care at home. Community medicine plays an important role in healthcare. It minimizes the impact of disability on the patients’ lives, maximizes their residual functions, improves their life qualities and restores their roles and functions in family and society (13). This could serve as an example of excellent nursing. As reported by Oeramman, indicators of excellent nursing include care and concern, professionalism, patient education of professional nursing, and improvement of patients’ quality of life.
In this case, owing to the long course and fluctuation of the disease, the visiting nurses adopted different roles in different conditions: caregiver, educator, consultant, and observer. They carried out individualized effective actions. With continuous deepening of health education, patient’s quality of life could be improved. The active participation of the patient’s family brought a hope for the prognosis. Social harmony increased the social recognition for nursing work, and upgraded the value of nurses.
In conclusion, nurses should put effort into community nursing (14) in order to allow patients to live in a safe environment, to satisfy the health needs of human being and their needs for health knowledge, and enhance their self-care abilities, which could further extend the intension of nursing care and bring it closer to society (15).
Acknowledgements
The study was supported by National Natural Science Foundation of China (81200936), Fudan University Research Fund for nursing (FNF201024), and 2011 Shanghai Medical College Young Scientist Fund of Fudan University (11L-24).
Disclosure: The authors declare no conflict of interest.
References
- Chen CF. Community nursing intervention of post-discharge rehabilitation of stroke patients. The Journal of Medical Theory And Practice 2011;20:2477-8.
- Dong ZL. The effect of PDCA cycle-type home nursing intervention on subjective well-being and life quality of coronary heart disease patients. Int J Nurs 2011;30:29-31.
- Zhu P, Zhou XX, Lin LL. Effect of telephone follow-up on the whole-process education for intrauterine adhesion patients after discharge. Journal of Nurses Training 2005;11:1003-4.
- Philip J, Collins A, Brand CA, et al. Health care professionals’ perspectives of living and dying with primary malignant glioma: Implications for a unique cancer trajectory. Palliat Support Care 2013;21:1-9. [Epub ahead of print]. [PubMed]
- Boele FW, Hoeben W, Hilverda K, et al. Enhancing quality of life and mastery of informal caregivers of high-grade glioma patients: a randomized controlled trial. J Neurooncol 2013;111:303-11. [PubMed]
- Sterckx W, Coolbrandt A, Dierckx de Casterlé B, et al. The impact of a high-grade glioma on everyday life: a systematic review from the patient’s and caregiver's perspective. Eur J Oncol Nurs 2013;17:107-17. [PubMed]
- Zhang XR, Zeng XY, Liang MY. Effect of community nursing intervention on the quality of life of stroke patients. Journal of Qilu Nursing 2011;17:23-4.
- Whisenant M. Informal caregiving in patients with brain tumors. Oncol Nurs Forum 2011;38:E373-81. [PubMed]
- Davis ME, Stoiber AM. Glioblastoma multiforme: enhancing survival and quality of life. Clin J Oncol Nurs 2011;15:291-7. [PubMed]
- Cahill JE, Armstrong TS. Caring for an adult with a malignant primary brain tumor. Nursing 2011;41:28-33. [PubMed]
- Wang H. Importance of community medical institution on health education. Journal of Shanxi Medical College for Continuing Education 2009;4:96.
- Zhang FX, Zhang WJ, Ju CF. Nursing of patients with Alzheimer’s disease. Journal of Weifang Medical College 2010;32:318-9.
- Tastan S, Kose G, Iyigun E, et al. Experiences of the relatives of patients undergoing cranial surgery for a brain tumor: a descriptive qualitative study. J Neurosci Nurs 2011;43:77-84. [PubMed]
- Huang J, Yang H, Liu JM. Impact of community nursing intervention on cervical spinal disease. Hunan Journal of Traditional Chinese Medicine 2011;6:74-5.
- Heese O, Vogeler E, Martens T, et al. End-of-life caregivers’ perception of medical and psychological support during the final weeks of glioma patients: a questionnaire-based survey. Neuro Oncol 2013;15:1251-6. [PubMed]