
Solitary rib metastasis of nasopharyngeal carcinoma
Introduction
Nasopharyngeal carcinoma could be considered an uncommon tumor in the United States and in Europe (1 to 14 cases per 100,000 people) in comparison to endemic areas, such as China and Hong Kong (25 to 50 cases per 100,000 people) (1,2). Most nasopharyngeal carcinomas are of epithelial origin and strongly associated with Epstein-Barr virus (EBV). Due to rich submucosal lymphatic system of nasopharynx, more than 70% of patients have clinically involved lymph nodes at initial diagnosis. The risk of distant metastasis is not related to tumor stage, but correlates strongly with clinical lymph-node stage. Bone metastasis from nasopharyngeal carcinoma represented the most common type of distant metastasis, followed closely by lung and liver (3). Skeleton metastatic sites are usually multifocal and commonly cause pain, resulting in immobility, anxiety and depression and this condition severely affects patient’s quality of life. We report a case of a 49-year-old man who developed solitary metastasis to the rib.
Case report
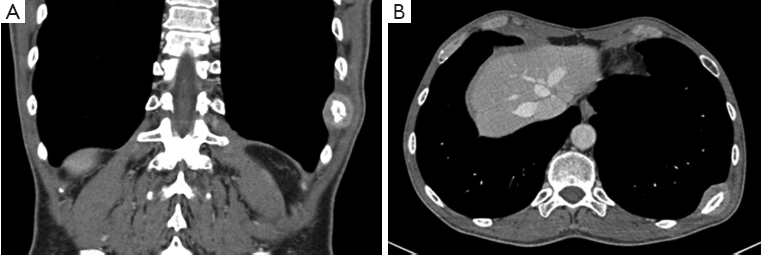
A 49-year-old Caucasian man received cisplatin-based chemotherapy (100 mg/m2, d 1-21) concurrently with definitive radiation therapy (total dose of 63.8 Gy, 220 cGy/fr) for a locally advanced cT2cN2cMx nasopharyngeal carcinoma in January 2012. Biopsy histological examination revealed an undifferentiated non-keratinizing carcinoma of the nasopharynx (WHO type III). By the end of radio-chemotherapy, the patient was clinically complete responder and followed by serial imaging until December 2012, when he presented a painful posterior chest tumefaction. In order to eliminate the possibility of multiple nasopharyngeal metastasis, a chest-abdominal scan and a bone scintigraphy were arranged. The chest-abdominal CT scan revealed only a solid mass, localized in the posterior arch of 10th left rib, with cortex erosion and invasion to the adjacent soft tissues (Figure 1). CT scanning did not reveal any cervical lymph node involvement in the neck area. Bone scintigraphy showed only an increased tracer uptake in the same skeleton position. A biopsy of the mass was performed. It was consistent with a nasopharyngeal metastasis: the histological features and staining pattern of the tumor cells revealed a metastatic carcinoma with morphological and immunophenotypical characteristics similar to those of the primary tumor. Adjuvant platinum-based chemotherapy was administered after radiation therapy of the metastatic site (total dose of 60 Gy, 200 cGy/fr). We are waiting for control contrast-enhanced CT scan.
Discussion
As mentioned, nasopharyngeal carcinoma is a common neoplasm in Southern China and Southeast Asia and, therefore, is often suspected as most of data analysis for therapeutic interventions, in nasopharyngeal carcinoma management, which are carried out in these endemic areas. Failure of treatment often arises because of distant metastases, which represent therefore an important survival factor. Despite the advancement in treatment optimization, the incidence of distant metastasis from nasopharyngeal carcinoma remains high and ranges from 15% to even 57% in N3 disease at diagnosis (4-8). The predilection of this cancer to develop skeletal metastases is widely confirmed in literature: the axial skeleton is the most common site of distant bone metastasis, with metastasis most frequently occurring in the spine and pelvis. The first region of involvement was lumbar spine (28.4%), then dorsal spine (27.7%), sacrum and pelvis (16.3%), femur (9.9%), and rib and sternum (7.8%) (9-11). Although the sites of distant metastases to the bone are clearly established, it is quite rare to see a solitary bone metastases in nasopharyngeal carcinoma (4). Moreover, an isolated rib bone involvement, in the absence of locoregional recurrence after achieving a complete response to aggressive multimodal treatment, with radiotherapy and chemotherapy, has been never reported. The role of surgical management of metastasis is weak and it is generally accepted that nasopharyngeal carcinoma disseminates early and the evidence available shows that salvage treatment strategy is best obtained using platinum-based chemotherapy (8).
To manage the single bone metastasis, considering the good performance status of the patient, we decided to treat the lesion with a local radiotherapy followed by chemotherapy: the goal was to improve quality of life and to prolong survival.
In conclusion, solitary rib metastases have been encountered rarely in nasopharyngeal carcinoma. We believe that local radiotherapy followed by chemotherapy provides an acceptable benefit in terms of palliation.
Acknowledgements
Disclosure: The authors declare no conflict of interest.
References
- Brennan B. Nasopharyngeal carcinoma. Orphanet J Rare Dis 2006;1:23. [PubMed]
- Pua KC, Khoo AS, Yap YY, et al. Nasopharyngeal Carcinoma Database. Med J Malaysia 2008;63:59-62. [PubMed]
- Leung SF, Teo PM, Shiu WW, et al. Clinical features and management of distant metastases of nasopharyngeal carcinoma. J Otolaryngol 1991;20:27-9. [PubMed]
- Cao X, Han Y, He L, et al. Risk subset of the survival for nasopharyngeal carcinoma patients with bone metastases: who will benefit from combined treatment? Oral Oncol 2011;47:747-52. [PubMed]
- Delis S, Biliatis I, Bourli A, et al. Surgical resection of a solitary liver metastasis from nasopharyngeal carcinoma: a case report. Hepatobiliary Pancreat Dis Int 2006;5:610-2. [PubMed]
- Razak AR, Siu LL, Liu FF, et al. Nasopharyngeal carcinoma: the next challenges. Eur J Cancer 2010;46:1967-78. [PubMed]
- Toh CK, Heng D, Ong YK, et al. Validation of a new prognostic index score for disseminated nasopharyngeal carcinoma. Br J Cancer 2005;92:1382-7. [PubMed]
- Huang PH, Shyng YC, Sloan P, et al. Nasopharyngeal carcinoma metastatic to the mandible. Open Dent J 2010;4:195-7. [PubMed]
- Sham JS, Cheung YK, Chan FL, et al. Nasopharyngeal carcinoma: pattern of skeletal metastases. Br J Radiol 1990;63:202-5. [PubMed]
- Khor TH, Tan BC, Chua EJ, et al. Distant metastases in nasopharyngeal carcinoma. Clin Radiol 1978;29:27-30. [PubMed]
- Ahmad A, Stefani S. Distant metastases of nasopharyngeal carcinoma: a study of 256 male patients. J Surg Oncol 1986;33:194-7. [PubMed]