
Oral cancer incidence and mortality in China, 2011
Introduction
Oral cancer is a part of group of head and neck cancer which may arise as a primary lesion in any part of the oral cavity or oropharynx. It most commonly involves the tongue, floor of the mouth, buccal mucosa, gingival, lips and oropharynx (1). Oral cancer is one of the most common cancers among head and neck neoplasms and it constitutes a major health problem particularly in developing countries (2). The International Agency for Research on Cancer (IARC) reported that there were 300,373 new cases and 145,353 deaths of oral cancer in 2012, accounting for approximately 2.1% of all new cancer cases and 1.9% of all cancer deaths in 2012, respectively. Most oral cancer incidence and mortality occurred in developing countries. Globally, the estimated 5-year prevalence of oral cancer is 702,149 (3).
Oral cancer is a life-threatening disease, almost 4.0-8.1% of females and 8.0-8.5% of males may develop oral cancer in their lives (4). The incidence of oral cancer has risen in the past decade and is usually recognized when symptomatic and at a late stage. The overall 5-year survival rates for oral cancer have remained low at approximately 50% for the past decades and have remained among the worst of all cancer death rates (5,6). Therefore, the burden of oral cancer is relatively high worldwide.
Incidence and mortality of oral cancer in China were not high. The cause of death survey in the 1990s and 2004-2005 in China showed that oral cancer only accounted for a small proportion of all malignancies. However, due to large population being in the risk of oral cancer such as tobacco smoking and alcohol consumption (7,8), the incidence and mortality of oral cancer are both increasing, although still in a low level. This indicates that much attention should be attracted in oral cancer.
Understanding the oral cancer incidence and mortality timely and accurately is the first step to prevent this malignancy. However, the data of incidence, distribution and mortality of oral cancer in the national level are limited among Chinese population at present. The National Cancer Registration Network collects information on cancer cases from population-based cancer registries in China each year since 1970s. The network is an information system designed for the collection, storage, management, and analysis of data on persons with malignant neoplasm with the purpose of helping to make decision regarding cancer prevention and control, usually covering a specific area. Using the data provided by cancer registry network, we estimated the incidence and mortality of oral cancer of 2011 in China in this study, addressing the issue of limited data on oral cancer. The information provided in this study will give clues to investigate the underlying cause of oral cancer and views for oral cancer preventive strategies.
Materials and methods
Incidence and mortality data
The National Central Cancer Registry of China (NCCR) is responsible for cancer data collection, evaluation and publication from local population-based cancer registries. The cancer information was reported to the cancer registries from local hospitals, and community health centers, including the Basic Medical Insurances for Urban Residents and the New-Rural Cooperative Medical System. The Vital Statistical Database was linked with the cancer incidence database for identifying cases with death certificate only (DCO) and follow-up. By 1 June 2014, 234 cancer registries (98 cities and 136 counties) from 31 provinces submitted 2011 data to the NCCR. Data covered about 221,390,275 people, accounting for about 16.43% of the national population. All cancer cases were classified according to the International Classification of Diseases for Oncology, 3rd edition (ICD-O-3) and the International Statistical Classification of Diseases and Related Health Problems 10th Revision (ICD-10). Invasive cases of oral cancer (ICD10: C00-10, C12-14) were extracted and analyzed from the overall cancer database.
Population data
The population was estimated based on the fifth National Population Census data [2000] provided by the National Statistics Bureau of China, taking into account of the changes of age composition, gender ratio and the proportion of urban and rural transformation released by the National Bureau of Statistics (http://data.stats.gov.cn/). The national population in 2011 was stratified by area (urban/rural), gender (male/female) and age groups (0-, 1-4, 5-84 by 5 years, 85+ years). The changes of age-specific death probability were also adjusted when calculating population. Linear changes were assumed in each age group between the 5th and 6th Population Census.
Quality control
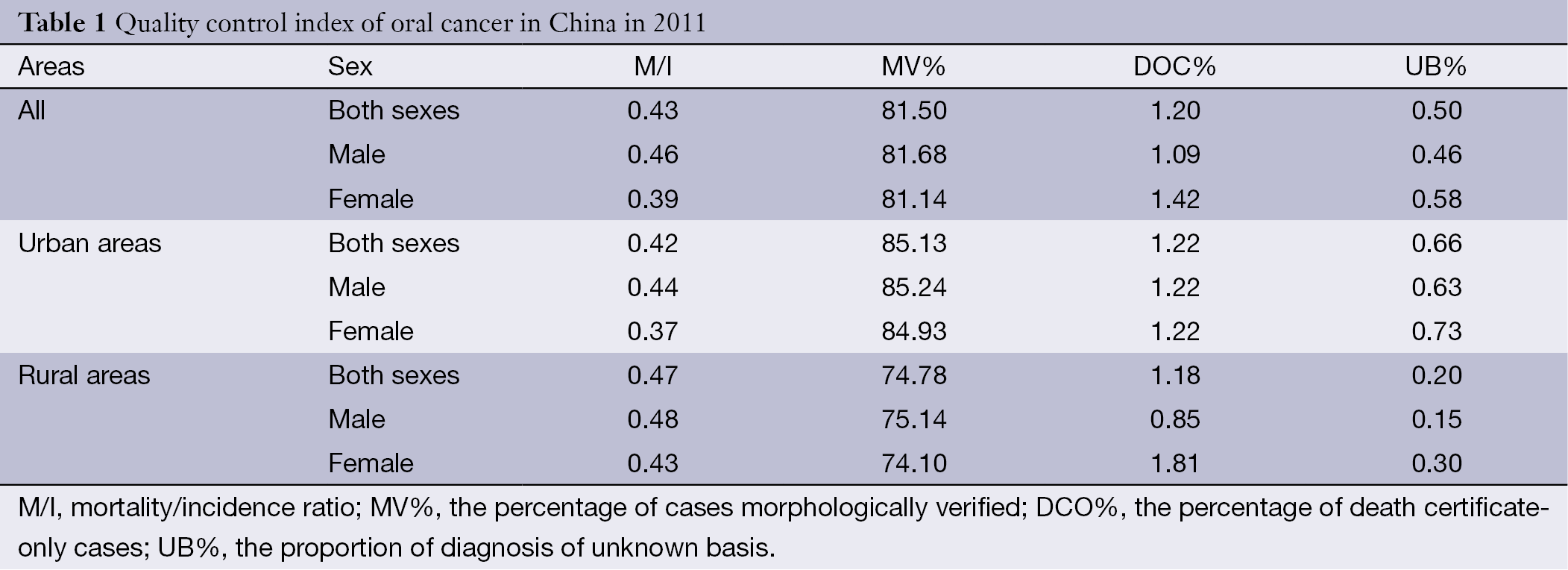
Each cancer registration data were checked and evaluated by NCCR based on “Guideline for Chinese Cancer Registration” and referring to relevant data quality criterion of “Cancer Incidence in Five Continents Volume IX” by International IARC/International Association of Cancer Registries (IACR). Proportion of morphologic verification (MV%), percentage of cancer cases identified with death certification only (DCO%), mortality to incidence ratio (M/I) and the proportion of diagnosis of unknown basis (UB%) were used to evaluate the completeness, validity and reliability of cancer statistics (9,10).
Statistical analysis
Incidence and mortality rates were calculated by area, gender and age groups. The numbers of new cases and deaths were estimated using the 5-year age-specific cancer incidence/mortality rates and the corresponding populations. The Chinese population in 2000 and World Segi’s population were used for age-standardized rates. The cumulative risk of developing or dying from cancer before 75 years of age (in the absence of competing causes of death) was calculated and presented as a percentage. Software including MS-Excel, IARCcrgTools2.05 issued by IARC and IACR was used for data checking and evaluation. SAS software (SAS Institute Inc., Cary, USA) was used to calculate the incidence and mortality rates.
Results
Data quality
Data from 177 population-based cancer registries distributed in 28 provinces were accepted for the annual report after evaluation based on quality control criteria in this study, covering a total of 175,310,169 populations and accounting for 13.01% of the overall national population in 2011. Among them, there were 88,655,668 males and 86,654,501 females. In the 177 accepted cancer registries, 77 registries were from urban areas and 100 registries were from rural areas, covering a population of 98,341,507 and 76,968,662, respectively.
The MV%, DCO%, M/I and UB% ratio of oral cancer for the national pooled data were 81.50%, 1.20%, 0.43 and 0.50%, respectively. In urban areas, the MV%, DCO%, M/I ratio and UB% were 85.13%, 1.22% 0.42 and 0.66%, compared to 74.78%, 1.18% 0.47 and 0.20% in rural areas. The detailed information of quality evaluation for oral cancers is presented in Table 1.
Full table
Incidence
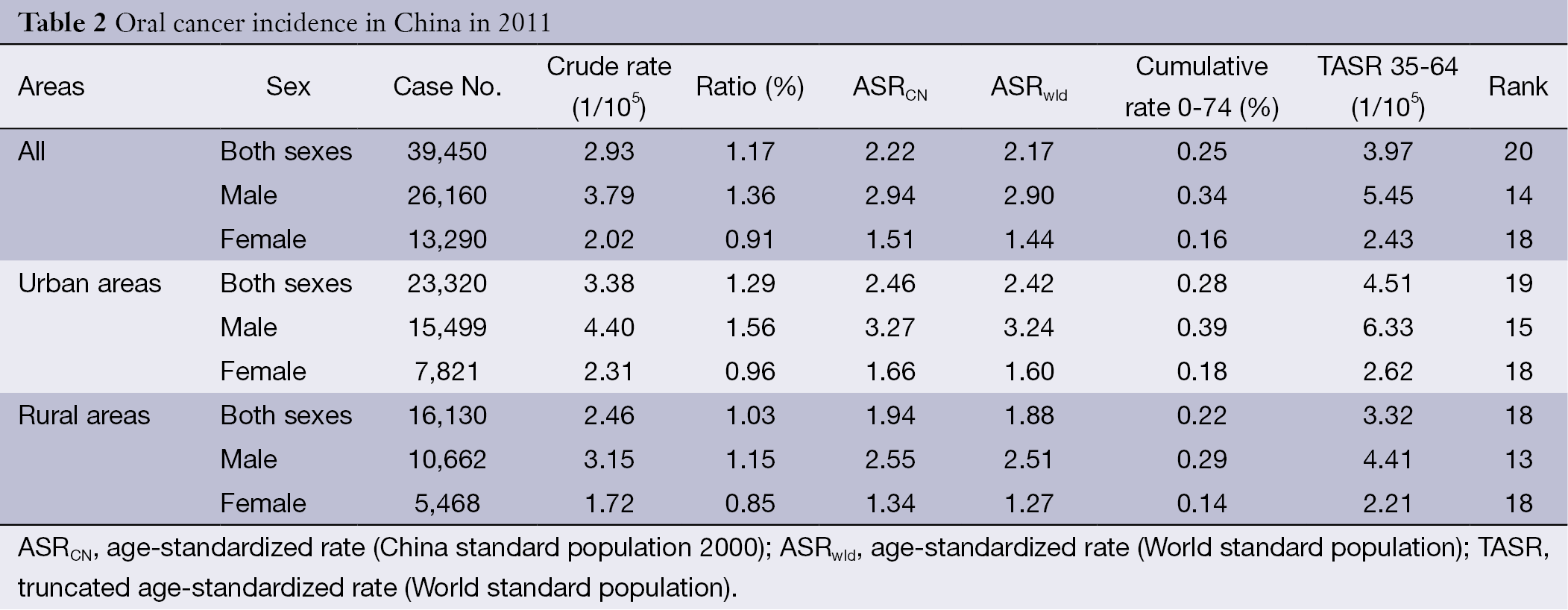
The estimate of new cases diagnosed with oral cancer was 39,450, including 26,160 males and 13,290 females. It accounted for 1.17% of all new cancer cases and ranked the twentieth most common cancer in 2011. The overall crude incidence rate for oral cancer was 2.93/100,000. The age-standardized rates by China (ASRCN) population and by World population (ASRwld) were 2.22/100,000 and 2.17/100,000, respectively. Among subjects aged 0-74 years, the cumulative incidence rate was 0.25%.
Oral cancer occurred more often among males than females. For males, a total of 26,160 new oral cancer cases were estimated to occur in 2011, which accounted for 1.36% of all new cancer cases and ranked the fourteenth most common cancer in males. The crude incidence rate for males was 3.79/100,000, whereas the ASRCN and ASRwld were 2.94/100,000 and 2.90/100,000, respectively. For females, a total of 13,290 new oral cancer cases were estimated to occur in 2011, which accounted for 2.02% of all new cancer cases and ranked the eighteenth most common cancer in females. The crude incidence rate for females was 2.02/100,000, whereas the ASRCN and ASRwld were 1.51/100,000 and 1.44/100,000, respectively. The crude incidence rate in urban areas was 3.38/100,000 and was higher than that in rural areas (2.46/100,000). After age standardization, the incidence rate in urban (2.42/100,000 for ASRwld) was still higher than that in rural areas (1.88/100,000 for ASRwld) (Table 2).
Full table
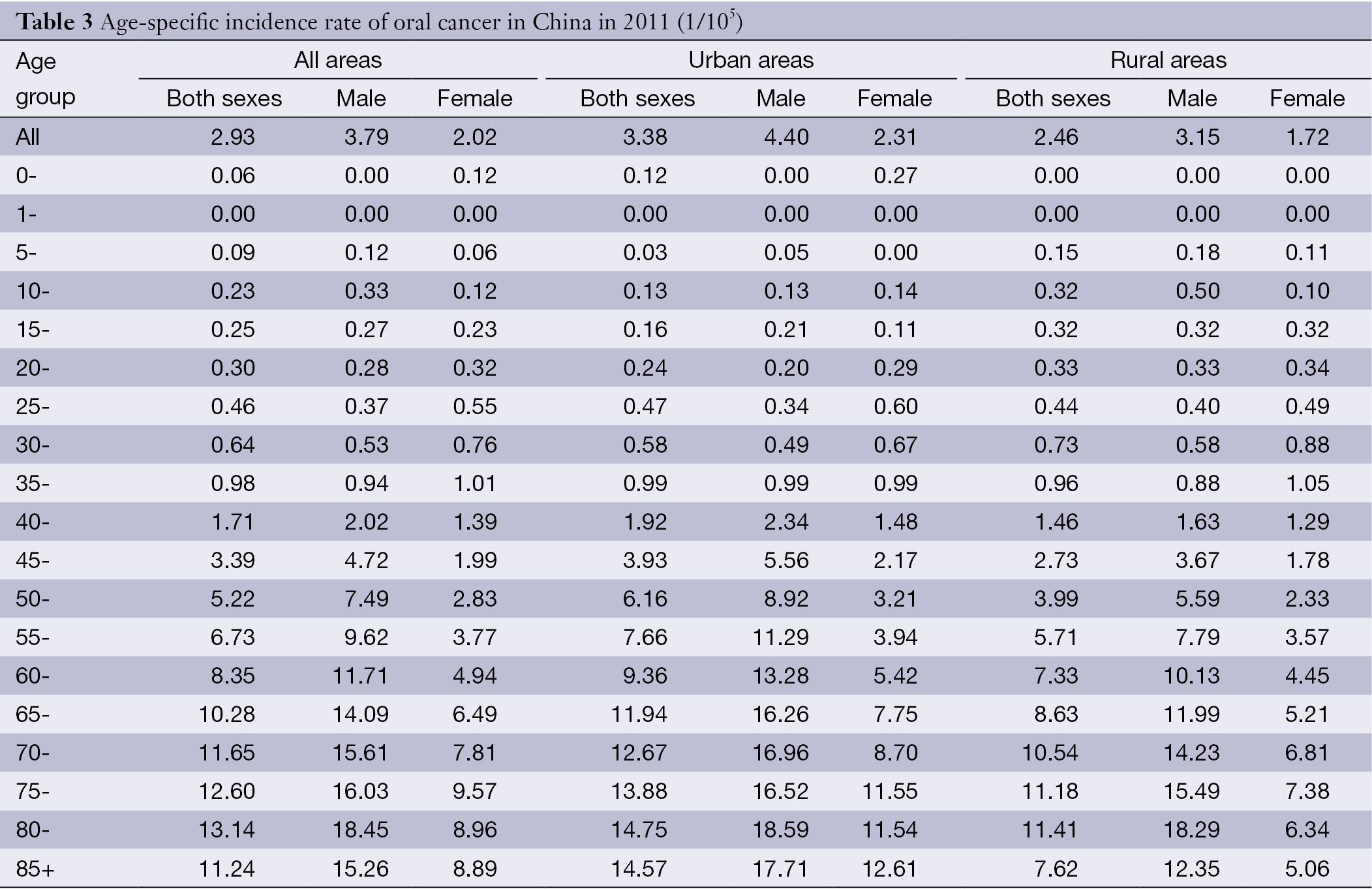
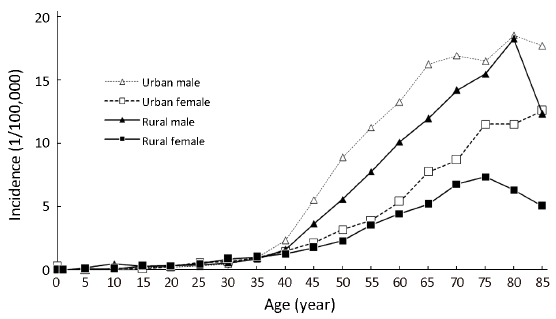
Overall, the age-specific incidence rate was relatively low in subjects before 40 years old. However, the rate was dramatically increasing after 40 years old, reaching peak for subjects of 80-84 years old (13.14/100,000). Generally, males had a higher age-specific incidence rate of oral cancer than females. With respect to the highest age-specific rates, it appeared in the age group of 80-84 years old for males and the age group of 75-79 years old for females. Stratified by area, the age-standardized oral cancer rates in urban areas were generally higher than that in rural areas, especially in older age groups (Table 3, Figure 1).
Full table
Mortality
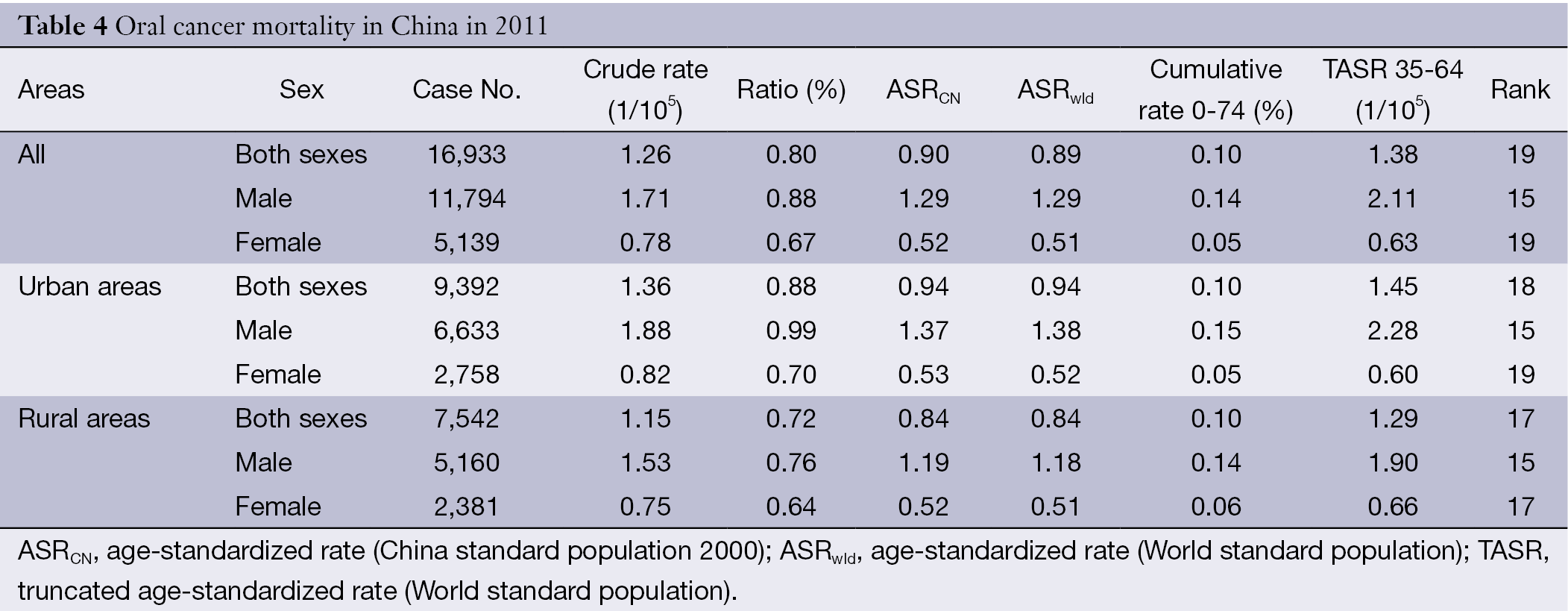
The estimated number of oral cancer deaths of China in 2011 was 16,933, including 11,794 males and 5,139 females. The overall crude mortality rate was 1.26/100,000, accounting for 0.80% of all cancer deaths, ranking nineteenth leading cause of cancer death. After age standardization by China population and World population, the standardized rates were 0.90/100,000 and 0.89/100,000, respectively. Among subjects aged 0-74 years, the cumulative mortality rate was 0.10%.
The mortality rate of oral cancer was much higher in males than in females. For males, there were 11,794 oral cancer deaths in 2011, which accounted for 0.88% of all cancer deaths and ranked the 15th leading cause of cancer death in males. The crude mortality rate for males was 1.71/100,000, whereas the ASRCN and ASRwld were both 1.29/100,000. For females, 5,139 oral cancer deaths were estimated to occur in 2011, which accounted for 0.67% of all cancer deaths and ranked the 19th leading cause of cancer death in females. The crude incidence rate for females was 0.78/100,000, whereas the ASRCN and ASRwld were 0.52/100,000 and 0.51/100,000, respectively. In urban areas, the crude rate, ASRCN and ASRwld were 1.36/100,000, 0.94/100,000 and 0.94/100,000. In rural areas, they were 1.15/100,000, 0.84/100,000 and 0.84/100,000, lower than those in urban areas (Table 4).
Full table
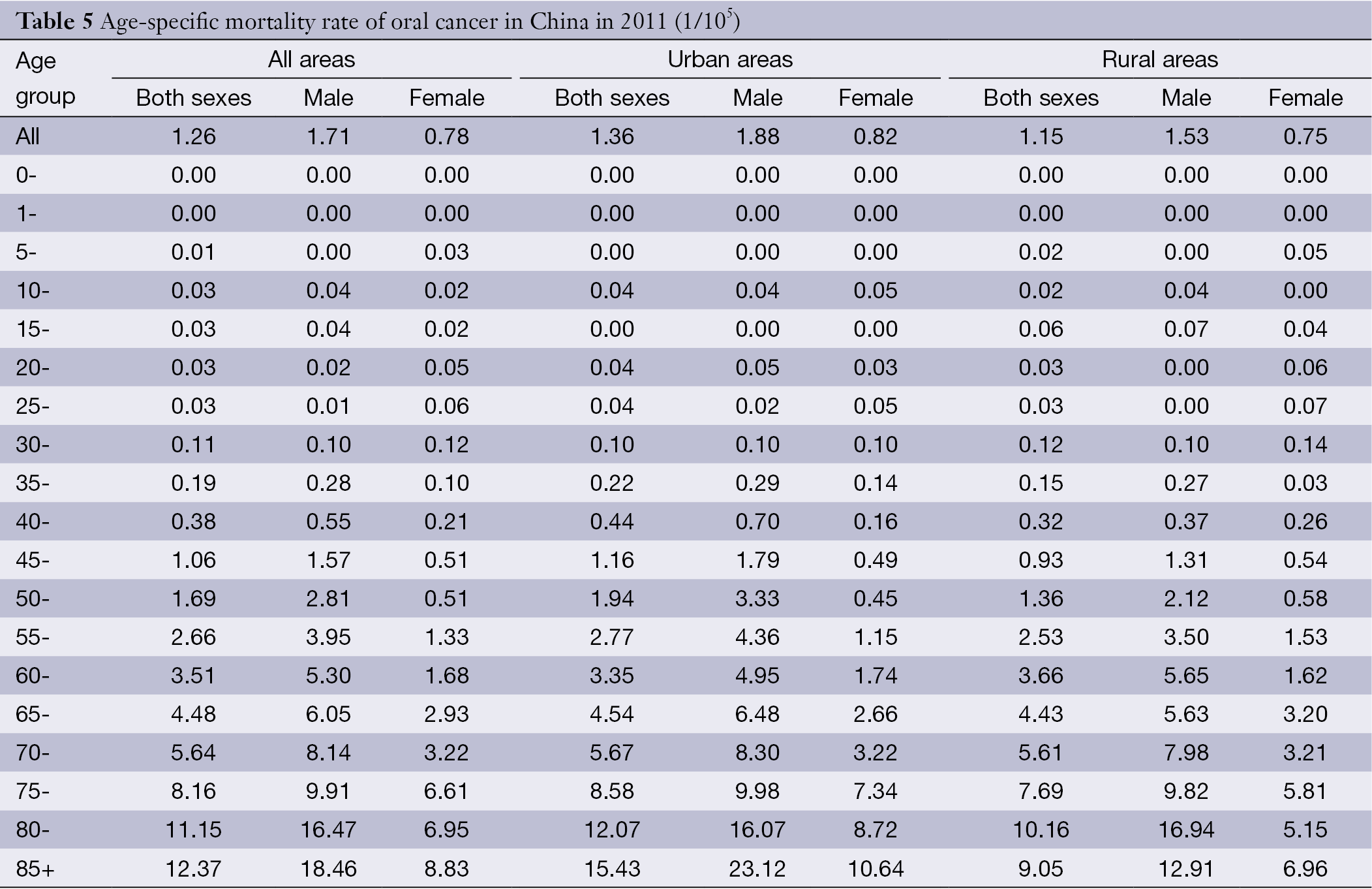
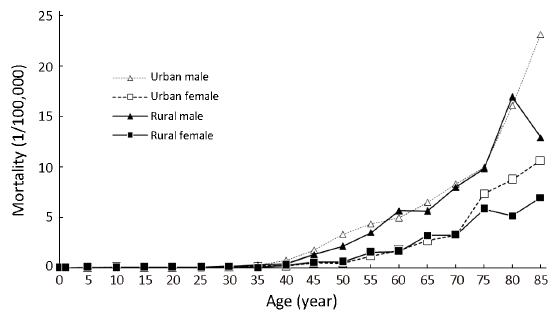
Age-specific mortality rates by gender and area are shown in Table 5 and Figure 2. Overall, the age-specific mortality rate was relatively low in age groups before 45 years old. However, the rate was dramatically increasing after 40 years old, reaching peak in the age group of 85 years or above (12.37/100,000). Similar to the incidence, males had a higher age-specific mortality rate of oral cancer than females. With respect to the highest age-specific rates, both males and females had the highest rates in the age group of 85 years old or above. Stratified by area, the age-standardized oral cancer rates in urban areas were generally higher than that in rural areas except for subjects in small age groups.
Full table
Discussion
In this study, we described the incidence and mortality rates of oral cancer among Chinese population in 2011 based on the data provided by cancer registry network, stratified by gender and area. The age-adjusted rates and age trends were also investigated. Results showed that the crude incidence and mortality rates of oral cancer were 3.79/100,000 and 1.26/100,000, respectively, which accounted for 1.36% of all new cancer cases and 0.88% of all cancer deaths in 2011. The age-standardized incidence and mortality rates by World population were 2.17/100,000 and 0.89/100,000. Oral cancer was more common in males and in urban areas.
Based on the data of GLOBOCAN 2012 (3), the ASR world incidence and mortality of oral cancer were 4.00/100,000 and 1.90/100,000 in the world, 3.7/100,000 and 2.1/100,000 in developing countries, 4.7/100,000 and 1.4/100,000 in developed countries, and 3.8/100,000 and 2.2/100,000 in Asia, respectively. There is a wide geographic variation in the incidence and mortality of oral cancer and nearly 70% of the oral cancer burden suffered by developing countries. The areas with the highest incidences and mortalities were South-Central Asia (ASRwld, 7.3/100,000 and 4.7/100,000), Melanesia (19.0/100,000 and 12.0/100,000), Central and Eastern Europe (5.0/100,000 and 2.6/100,000) and Eastern Africa (3.6/100,000 and 2.5/100,000). With regard to high risk countries of oral cancer, Papua New Guinea (ASRwld, 25.0/100,000 and 16.0/100,000), Pakistan (9.8/100,000 and 5.9/100,000), Sri Lanka (10.3/100,000 and 3.5/100,000), Maldives (11.0/100,000 and 4.1/100,000), and Bangladesh (9.4/100,000 and 5.6/100,000) were countries with the highest incidence and mortality rates. Compared with these data, the results of our study showed that oral cancer incidence and mortality were lower in China than the world’s and Asian’s level, indicating that oral cancer burden in China is not high. Consistent with other studies which showed that males had a higher incidence and mortality rates than females (6,11), our study also showed this trend.
Oral cancer is a disease of multi-factorial origin and risk factors vary and operate differently for different population groups (12). However, tobacco use and alcohol consumption are regarded as the primary risk factors for oral carcinoma (13-15). Jaber reported that individuals who smoke more than 20 cigarettes a day and consumed more than 100 g of alcohol a day were believed to be at increased risk for oral epithelial dysplasia (16). In addition, alcohol has been found to be an independent risk factor for oral cancer among nonsmokers and tobacco smoking in non-drinkers (17). Moreover, both factors together seem to enhance the carcinogenic effect (18). Yang and Ma reported men with the habit of smoking and drinking in China consisted of 60% and 40% of the whole population of males (7,8). These can explained that why oral cancer was more common in males and in urban areas in China. Chewing betel quid was also a main risk factor of oral cancer in some areas (15). Gupta suggests the incidence rates are reaching high proportions possibly due to the availability of manufactured areca nut products (19). This rising incidence is most strongly seen in developing countries in South-Central Asia, where oral cavity is often the first or second most common site for malignant cancer (20). Aging is positively correlated with the incidence of oral cancer. From our study, we could observe that the oral cancer incidence and mortality rates were positively correlated with the growing of age. Recently years, the majority of research on the changing epidemiology has focused on the human papilloma virus (HPV) and its association with oral cancer. The HPV involvement in oral carcinogenesis was first proposed in 1983 by Syrjänen et al. (21). An analysis of Swedish Cancer registry data showed that husbands of women with cervical carcinoma had a significantly increased risk of developing either base of tongue or tonsil cancer (22). Since HPV is involved in the development of some oral cancers, the implementation of a vaccine program may prove to be beneficial in preventing not only cervical cancer, but possibly HPV-positive oral cancers as well.
As we know, most cancers and their related complications are preventable through early detection. Unfortunately, oral premalignant disorders are usually misdiagnosed (4). This is in part due to the lack of training of health professionals for early detection and diagnosis. Despite significant advances in cancer treatment, early detection of oral cancer and its curable precursors remain the best way to ensure patient survival and improved quality of life. Therefore, improvement of physicians’ or dentists’ level of knowledge about oral potentially malignant disorders may play a key role in saving patients’ lives (23). Besides, choosing the appropriate method is also a critical step for the early detection of oral cancer (23,24). Devices to assist in detection and promote diagnostic procedures included toluidine blue dye, exfoliative cytologic techniques, salivary diagnostics and optical imaging systems (25).
Conclusions
This study depicted the incidence and mortality of oral cancer among Chinese population in 2012. Although oral cancer burden of China is not high, we must pay attention to this malignancy as well. Date in the study may have important implication for oral cancer prevention and research, despite the data may have some flaws. In the next step, we will improve the coverage and quality of cancer registry, providing more accurate results for cancers. In addition, further studies need to be done for primary and secondary prevention research of oral cancer, especially for the high risk population.
Acknowledgements
Disclosure: The authors declare no conflict of interest.
References
- Masthan KM, Babu NA, Dash KC, et al. Advanced diagnostic aids in oral cancer. Asian Pac J Cancer Prev 2012;13:3573-6. [PubMed]
- Johnson NW, Warnakulasuriya S, Gupta PC, et al. Global oral health inequalities in incidence and outcomes for oral cancer: causes and solutions. Adv Dent Res 2011;23:237-46. [PubMed]
- All Cancers (excluding non-melanoma skin cancer) Estimated Incidence, Mortality and Prevalence Worldwide in 2012. Available online: http://globocan.iarc.fr/Pages/fact_sheets_cancer.aspx
- Mortazavi H, Baharvand M, Mehdipour M. Oral potentially malignant disorders: an overview of more than 20 entities. J Dent Res Dent Clin Dent Prospects 2014;8:6-14. [PubMed]
- Adami GR, Adami AJ. Looking in the mouth for noninvasive gene expression-based methods to detect oral, oropharyngeal, and systemic cancer. ISRN Oncol 2012;2012:931301.
- Messadi DV. Diagnostic aids for detection of oral precancerous conditions. Int J Oral Sci 2013;5:59-65. [PubMed]
- Yang GH, Ma JM, Liu N, et al. Smoking and passive smoking in Chinese, 2002. Chinese Journal of Epidemiology 2005;26:77-83. [PubMed]
- Ma GS, Zhu DH, Hu XQ, et al. The drinking practice of people in China. Acta Nutrimenta Sinica 2005;27:362-5.
- Curade MP, Edwards B, Shin HR, et al. eds. Cancer Incidence in Five Continents Vol. IX. Lyon: IARC Scientific Publications, 2008.
- Parkin DM, Chen VW, Ferlay J, et al. eds. Comparability and quality control in cancer registration. Lyon: IARC Technical Report, 1994.
- Brocklehurst P, Kujan O, O'Malley LA, et al. Screening programmes for the early detection and prevention of oral cancer. Cochrane Database Syst Rev 2013;11:CD004150. [PubMed]
- Gupta B, Johnson NW. Systematic review and meta-analysis of association of smokeless tobacco and of betel quid without tobacco with incidence of oral cancer in South Asia and the Pacific. PLoS One 2014;9:e113385. [PubMed]
- Scully C, Petti S. Overview of cancer for the healthcare team: aetiopathogenesis and early diagnosis. Oral Oncol 2010;46:402-6. [PubMed]
- Gupta B, Ariyawardana A, Johnson NW. Oral cancer in India continues in epidemic proportions: evidence base and policy initiatives. Int Dent J 2013;63:12-25. [PubMed]
- Lambert R, Sauvaget C, de Camargo Cancela M, et al. Epidemiology of cancer from the oral cavity and oropharynx. Eur J Gastroenterol Hepatol 2011;23:633-41. [PubMed]
- Jaber MA. Oral epithelial dysplasia in non-users of tobacco and alcohol: an analysis of clinicopathologic characteristics and treatment outcome. J Oral Sci 2010;52:13-21. [PubMed]
- Hashibe M, Brennan P, Benhamou S, et al. Alcohol drinking in never users of tobacco, cigarette smoking in never drinkers, and the risk of head and neck cancer: pooled analysis in the International Head and Neck Cancer Epidemiology Consortium. J Natl Cancer Inst 2007;99:777-89. [PubMed]
- Majchrzak E, Szybiak B, Wegner A, et al. Oral cavity and oropharyngeal squamous cell carcinoma in young adults: a review of the literature. Radiol Oncol 2014;48:1-10. [PubMed]
- Gupta PC. Mouth cancer in India: a new epidemic? J Indian Med Assoc 1999;97:370-3. [PubMed]
- Sinha R, Daniel CR, Devasenapathy N, et al. Multi-center feasibility study evaluating recruitment, variability in risk factors and biomarkers for a diet and cancer cohort in India. BMC Public Health 2011;11:405. [PubMed]
- Syrjänen KJ, Pyrhönen S, Syrjänen SM, et al. Immunohistochemical demonstration of human papilloma virus (HPV) antigens in oral squamous cell lesions. Br J Oral Surg 1983;21:147-53. [PubMed]
- Hemminki K, Dong C, Frisch M. Tonsillar and other upper aerodigestive tract cancers among cervical cancer patients and their husbands. Eur J Cancer Prev 2000;9:433-7. [PubMed]
- Warnakulasuriya S, Johnson NW, van der Waal I. Nomenclature and classification of potentially malignant disorders of the oral mucosa. J Oral Pathol Med 2007;36:575-80. [PubMed]
- Farah CS, McCullough MJ. A pilot case control study on the efficacy of acetic acid wash and chemiluminescent illumination (ViziLite) in the visualisation of oral mucosal white lesions. Oral Oncol 2007;43:820-4. [PubMed]
- Güneri P, Epstein JB. Late stage diagnosis of oral cancer: components and possible solutions. Oral Oncol 2014;50:1131-6. [PubMed]