
Presentation delay in breast cancer patients and its association with sociodemographic factors in North Pakistan
Introduction
Breast cancer is the most frequent malignancy among women in Pakistan with a high grade and a late stage of presentation probably due to lack of screening and awareness programs. Jamal et al. in their analytical study that the pattern of malignancies in Pakistan is changing with breast cancer coming at the top among females, similar trend was found in other studies which also highlighted scarcity of diagnostic and treatment facilities for these patients in Pakistan (1-5). The impact of delays on survival between the onset of symptoms and the start of treatment is controversial and cannot be studied in randomized controlled trials due to ethical reasons. In another study, Richards et al. found that there is evidence that patients with delays of 12-26 weeks had significantly worse survival rates than those with delays of less than 12 weeks (6). Richards et al. did a tremendous attempt by conducting a systematic review of 87 observational studies across the globe (101,954 patients) to assess the impact of delays on survival. They founds that delays of 3-6 months are associated with lower survival (7). In another study conducted by Kothari A and Fentiman IS, designed to control for the lead-time bias, it was found that that survival measured from both date of diagnosis and onset of patient’s symptoms was worse in women with delays of >12 weeks (8). Poverty, social culture and lack of awareness about the disease and its management in our region may be the factors leading to misconception and false beliefs among these women resulting in delayed presentation. The concept of the study was based on our observations during our routine clinical practice. It is written for publication with intent to draw the attention of relevant stakeholders in our region. This will be helpful in devising sustainable strategies for health education of the targeted population and removing barriers towards early presentation to the doctor. Short term outcomes will be increased early detection rate with a long term impact of enhanced control over the disease and reduced overall burden in the region. The main objectives of this study were to determine the frequency of patients with breast lump who presented late to the doctor, to determine causes of delayed presentation and to determine the association of delayed presentation with age, family history, marital, menopausal, education and socioeconomic status.
Materials and methods
It was a cross-sectional study and was carried out at Nuclear Medicine, Oncology and Radiotherapy Institute (NORI), Islamabad, Pakistan. Data was collected over a period of 1 year (September 2012 to August 2013). Study design was approved by the hospital ethical committee. Informed consent was obtained from each patient with assurance of strict confidentiality for their valuable information. We interviewed 315 histologically confirmed breast cancer patients being managed at our institute. All those patients who were not willing to disclose their information about reasons of their delayed presentation were excluded from the study. Delay was defined as more than 3 months from appearance of symptoms to the consultation from expert physician. Data was stratified with respect to studied socio-demographic variables i.e., age (<40 or >40 years), family history (positive or negative), menopausal status (pre or post menopausal), education status (<8 or >8 school years) and socioeconomic status [poor-low (monthly income of PKR <15,000/month) or middle-high (PKR >15,000/month)]. Five questions were asked from each patient, which could reflect their understanding about the disease and which could be the likely reasons of their delayed presentation; questions were selected after review of the literature and keeping in view our social culture. The questions were: (I) Did you present late because you were using alternative medicines at traditional healers? (II) Did you present late due to painless lump; thought it was not dangerous enough to consult the expert physician? (III) Did you present late due to not having enough resources to pay the doctor; (IV) Did you feel shy to show breasts to male doctors with no access to female doctors in the surroundings? (V) Did you present late due to other reasons? Chi-square test was employed as a test of association between the variables and logistic regression analysis was performed to estimate adjusted odds ratios (OR) and confidence intervals (CI) of different socio-demographic variables and their independent influence on delayed presentation.
Results
A total of 315 female patients were interviewed during the study period at NORI Islamabad, Pakistan. Demographic characteristics of study sample are summarized in Table 1. A total of 39.01% (n=123) of patients presented late according to our definition. Out of 100% (n=123) of patients who presented late, 40.7% (n=50) wasted time using alternative medicines at traditional healers; 25.2% (n=31) thought treatment was expensive and they were not having enough resources; 17.1% (n=21) thought it was not dangerous enough to consult the doctor due to painless nature of the disease; 10.6% (n=13) felt shyness to show breast to male doctors with no access to female doctors in the surroundings and 6.5% (n=8) presented late due to other reasons (pregnant or lactating at that time). Higher age group, less than 8 school years of education, low to middle socio-economic status and negative family history were significantly associated with delayed presentation (P<0.05), results are summarized in Table 1. Education and socioeconomic status were found to be two independent factors related to the delayed presentation after adjustment for other factors (OR of 2.26, 2.29 and 95% CI was 1.25-4.10, 1.06-4.94 respectively), results are summarized in Table 2.
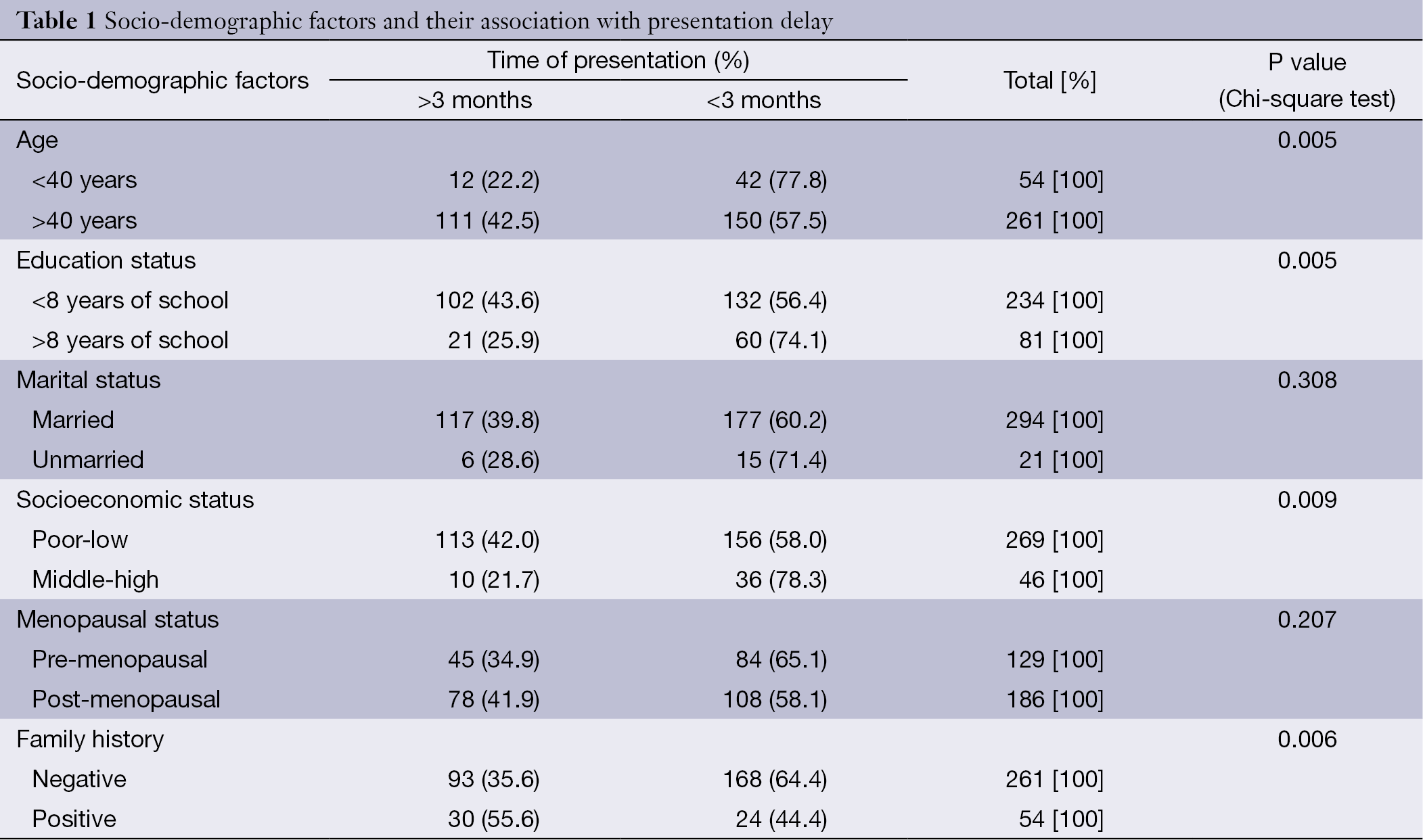
Full table
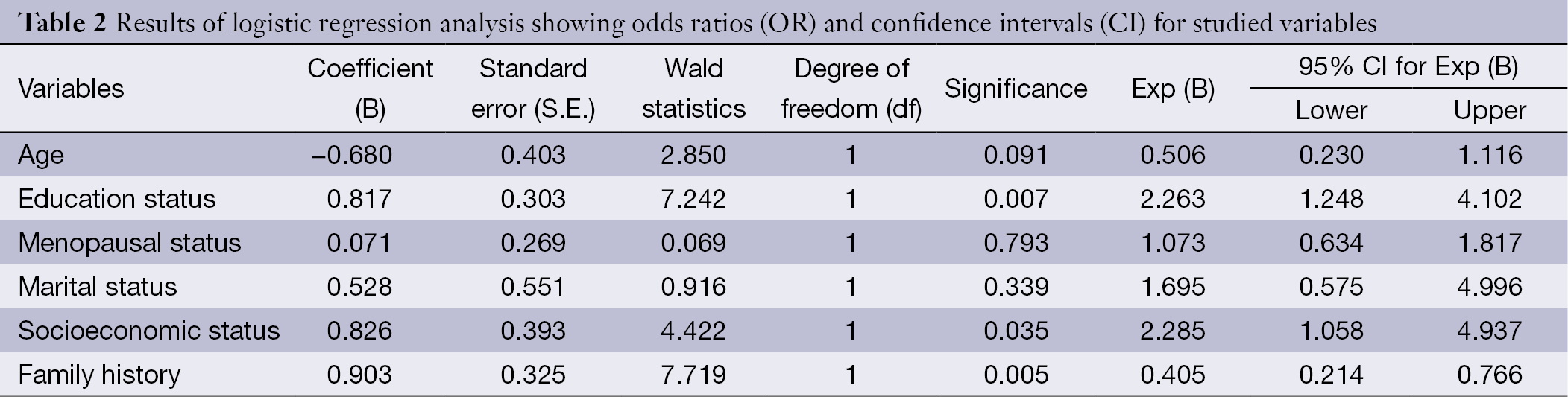
Full table
Discussion
There is always an interval between the first symptoms, time to diagnosis and start of treatment in women with symptomatic breast cancer. This interval can be divided into two components, patient and system delay. Patient delay is the time it takes for a woman to seek help once she has discovered a breast symptom. System delay is the time it takes for a woman to be evaluated, diagnosed and treated once she has sought help. A systematic review by Richards et al. showed that delays of 3-6 months were clearly associated with increased tumor size, advance in disease stage and poorer long-term prognosis (7). Nevertheless, controversy persists regarding the impact of delay on survival. The conflicting results may be due to a difference in sample characteristics, differences in the delay interval studied or variations in the definition of delay. Results of a more recent systemic review conducted at department of Community Health & Preventive Medicine, Morehouse School of Medicine, Atlanta, GA, USA showed that while earlier studies tended to show that increased delay is associated with more advanced stage cancers at diagnosis resulting in poorer survival rates, more recent ones showed mixed results. Some showed increased survival with longer delays, which could be due to diagnostic difficulties resulting in this survival paradox. A rapidly growing lump may suggest cancer to both doctors and patients, while a slow growing lump or other symptoms could be less obvious to them. If this is the case, then shorter delays would be seen with more aggressive tumors for which the prognosis is worse leading to reduced survival. It seems logical that a tumor that is more advanced at diagnosis would lead to shorter survival but several studies in that review highlighted that one should be very careful in making such assumptions, which could be even dangerous at times (8). Another major drawback of many studies was that the potential confounding effect of lead-time bias was not taken into account. One of the largest single institution studies conducted by Kothari and Fentiman, designed to control for the lead-time bias, confirmed that survival measured from both date of diagnosis and onset of patient’s symptoms was worse in women with delays of >12 weeks (9). It was important to identify groups of patients at high risk for presentation delay in our region in order to develop strategies for educating targeted groups. Present study was designed and conducted with the same concept. Our results revealed there were 39.01% of patients who presented late according to our definition (>3 months). Main reasons were using alternative medicines, lack of financial resources, painless nature of the disease and shyness. Higher age group, less than 8 school years of education, low to middle socio-economic status and negative family history were significantly associated with delayed presentation. Education and socioeconomic status were found to be two independent factors related to the delayed presentation after adjustment for other factors. Our findings are similar with the already published ones on the subject. In other studies conducted by Brzozowska et al. and other authors worldwide, it was found that the phenomenon of delayed presentation occurs across the globe with a range 14% to 73% (mean 33.1%±19.5% SD) of patients present late (>3 months) to the doctors. Most frequent reasons of delayed presentation in these studies were found to be painless nature of the lump, fear (partner abandonment, cancer treatment, disfigurement after surgery, chemotherapy), shyness, fatalism, using alternative therapies, denial and inaccessibility to healthcare services. Higher age groups, negative family history, low education and low socioeconomic status were found to be the factors associated with delayed presentation in these studies (10-30). Even in affluent societies women with fewer financial resources are more likely to delay seeking medical attention. In a recent prospective, multicenter cohort study conducted in USA, among women of ≤40 years of age with recently diagnosed breast cancer, 17% reported a self-delay which was associated with poorer financial status (31). Interestingly, paradoxical results are seen in lesser affluent societies. In a cross-sectional study conducted in Thailand, 180 women with invasive breast cancer were interviewed about potential risk factors and markers of delayed presentation. Results showed that 17% delayed seeking consultation for longer than 3 months, which was associated with higher family income and smoking (32). Association with higher income and smoking may be explained by a more casual attitude of these women towards their health problems; nevertheless, this is an example of complex interactions between psycho-social and cognitive factors which may not be fully explained with simple assumptions. In another study conducted on 129 African American women with self-detected breast symptoms in Atlanta, USA, influence of religiosity, spirituality, and cancer fatalism on delay in diagnosis and breast cancer stage was studied. Participants were found to be highly religious and spiritual but not fatalistic. An association was found between disclosing a breast symptom to God only and delay in seeking medical care. In contrast, women who had told a person about their breast symptom were more likely to seek medical care sooner. They were also more likely to present with a later stage of breast cancer than women who sought care within 3 months of symptom discovery (33). Although the phenomenon of religiosity and spirituality is quite common in our society, we did not include those variables in our study. These areas definitely need to be explored in future studies as religious and spiritual beliefs have an overwhelming influence on the help seeking attitudes of people in our society. Empowerment of women and fatalism are also other variables which could influence the time taken by women to present their breast symptoms to doctor. These issues need to be separately discussed in future studies.
The theme, derived from the study and after review of literature on the same subject, is that help-seeking behavior of women is not merely a matter of education and economics. It is also influenced by a complex interaction of psycho-social, environmental, cultural and cognitive factors. Healthcare system weakness with lack of coordination between public health and clinical service providers is also an important contributory factor influencing the help seeking behavior of the women with suspected breast cancer. Public health department has to do an enormous amount of work in this regard by creating communication network among all stakeholders with a goal of raising awareness levels of general population. An intense and focused awareness campaign is needed to educate the general population. The focus of awareness campaigns should be to communicate the people that the disease has a dangerously high level of incidence in Pakistan, the disease is curable and need not be made fatal, it can be detected early even by simple self-diagnosis methods and the life after cancer is worth living. We would also like to draw the attention of public health authorities for creation of network of other organizations working in the same direction and strengthening the base of this program nationwide. Training programs for Lady Health Workers across the country could be highly helpful for educating the people with early referral to tertiary care hospital. We recommend setting up dedicated breast clinics with essential diagnostic facilities in remote areas of the region for easy accessibility to healthcare services to women living there with lowest socio-economic status. Finally, we recommend clinical services providers in our region should assess whether a woman is the one in three who will delay the evaluation of her breast symptoms with appropriate interventions targeted to behavior modifications, creating awareness about advances in disease management and motivating them to stay with their complete treatment course.
Conclusions
A significant percentage of women with breast cancer in North Pakistan are experiencing presentation delay due to their misconceptions and false beliefs about the disease and its management. Coordinated efforts with public health department are needed to educate the focused groups and removing the barriers identified in the study. Long term impact will be in terms of increased survival rates in these patients with reduced overall burden of the disease in the region.
Acknowledgements
We would like to acknowledge all the studied patients for their cooperation. We wish to pay special gratitude to Dr. Javaid Irfan, Director NORI Islamabad and Dr. Mohammad Faheem, consultant Oncologist NORI Islamabad for his support and encouragement throughout the project. We also acknowledge our families and friends for their continuous support and motivation.
Disclosure: The authors declare no conflict of interest.
References
- Jamal S, Atique M, Khadim MT. Changing pattern of malignancies: analysis of histopathology based tumour registry data and comparison of three decades at Armed Forces Institute of Pathology, Rawalpindi, Pakistan. J Pak Med Assoc 2014;64:24-7. [PubMed]
- Khurshid A, Faridi N, Arif AM, et al. Breast lesions in adolescents and young women in Pakistan--a 5 year study of significance of early recognition. Asian Pac J Cancer Prev 2013;14:3465-7. [PubMed]
- Moore MA, Ariyaratne Y, Badar F, et al. Cancer epidemiology in South Asia - past, present and future. Asian Pac J Cancer Prev 2010;11:49-66. [PubMed]
- Bhurgri Y, Kayani N, Faridi N, et al. Patho-epidemiology of breast cancer in Karachi '1995-1997'. Asian Pac J Cancer Prev 2007;8:215-20. [PubMed]
- Naeem M, Khan N, Aman Z, et al. Pattern of breast cancer: experience at Lady Reading Hospital, Peshawar. J Ayub Med Coll Abbottabad 2008;20:22-5. [PubMed]
- Richards MA, Smith P, Ramirez AJ, et al. The influence on survival of delay in the presentation and treatment of symptomatic breast cancer. Br J Cancer 1999;79:858-64. [PubMed]
- Richards MA, Westcombe AM, Love SB, et al. Influence of delay on survival in patients with breast cancer: a systematic review. Lancet 1999;353:1119-26. [PubMed]
- Caplan L. Delay in breast cancer: implications for stage at diagnosis and survival. Front Public Health 2014;2:87. [PubMed]
- Kothari A, Fentiman IS. 22. Diagnostic delays in breast cancer and impact on survival. Int J Clin Pract 2003;57:200-3. [PubMed]
- Brzozowska A, Duma D, Mazurkiewicz T, et al. Reasons for delay in treatment of breast cancer detected due to breast self-examination in women from the Lubelskie region. Ginekol Pol 2014;85:14-7. [PubMed]
- Jones CE, Maben J, Jack RH, et al. A systematic review of barriers to early presentation and diagnosis with breast cancer among black women. BMJ Open 2014;4:e004076. [PubMed]
- Weinmann S, Taplin SH, Gilbert J, et al. Characteristics of women refusing follow-up for tests or symptoms suggestive of breast cancer. J Natl Cancer Inst Monogr 2005;35:33-8. [PubMed]
- Montazeri A, Ebrahimi M, Mehrdad N, et al. Delayed presentation in breast cancer: a study in Iranian women. BMC Womens Health 2003;3:4. [PubMed]
- Ermiah E, Abdalla F, Buhmeida A, et al. Diagnosis delay in Libyan female breast cancer. BMC Res Notes 2012;5:452. [PubMed]
- Norsa'adah B, Rampal KG, Rahmah MA, et al. Diagnosis delay of breast cancer and its associated factors in Malaysian women. BMC Cancer 2011;11:141. [PubMed]
- Ali R, Mathew A, Rajan B. Effects of socio-economic and demographic factors in delayed reporting and late-stage presentation among patients with breast cancer in a major cancer hospital in South India. Asian Pac J Cancer Prev 2008;9:703-7. [PubMed]
- Poum A, Promthet S, Duffy SW, et al. Factors associated with delayed diagnosis of breast cancer in northeast Thailand. J Epidemiol 2014;24:102-8. [PubMed]
- Gullatte MM, Phillips JM, Gibson LM. Factors associated with delays in screening of self-detected breast changes in African-American women. J Natl Black Nurses Assoc 2006;17:45-50. [PubMed]
- O'Mahony M, Hegarty J. Factors influencing women in seeking help from a health care professional on self discovery of a breast symptom, in an Irish context. J Clin Nurs 2009;18:2020-9. [PubMed]
- Innos K, Padrik P, Valvere V, et al. Identifying women at risk for delayed presentation of breast cancer: a cross-sectional study in Estonia. BMC Public Health 2013;13:947. [PubMed]
- Grunfeld EA, Hunter MS, Ramirez AJ, et al. Perceptions of breast cancer across the lifespan. J Psychosom Res 2003;54:141-6. [PubMed]
- Gullatte MM, Brawley O, Kinney A, et al. Religiosity, spirituality, and cancer fatalism beliefs on delay in breast cancer diagnosis in African American women. J Relig Health 2010;49:62-72. [PubMed]
- Gullatte MM, Hardin P, Kinney A, et al. Religious beliefs and delay in breast cancer diagnosis for self-detected breast changes in African-American women. J Natl Black Nurses Assoc 2009;20:25-35. [PubMed]
- O'Mahony M, McCarthy G, Corcoran P, et al. Shedding light on women's help seeking behaviour for self discovered breast symptoms. Eur J Oncol Nurs 2013;17:632-9. [PubMed]
- Gullate M. The influence of spirituality and religiosity on breast cancer screening delay in African American women: application of the Theory of Reasoned Action and Planned Behavior (TRA/TPB). ABNF J 2006;17:89-94. [PubMed]
- Meechan G, Collins J, Petrie KJ. The relationship of symptoms and psychological factors to delay in seeking medical care for breast symptoms. Prev Med 2003;36:374-8. [PubMed]
- Norsa'adah B, Rahmah MA, Rampal KG, et al. Understanding barriers to Malaysian women with breast cancer seeking help. Asian Pac J Cancer Prev 2012;13:3723-30. [PubMed]
- Bish A, Ramirez A, Burgess C, et al. Understanding why women delay in seeking help for breast cancer symptoms. J Psychosom Res 2005;58:321-6. [PubMed]
- Li WW, Lam WW, Wong JH, et al. Waiting to see the doctor: understanding appraisal and utilization components of consultation delay for new breast symptoms in Chinese women. Psychooncology 2012;21:1316-23. [PubMed]
- O'Mahony M, Hegarty J, McCarthy G. Women's help seeking behaviour for self discovered breast cancer symptoms. Eur J Oncol Nurs 2011;15:410-8. [PubMed]
- Ruddy KJ, Gelber S, Tamimi RM, et al. Breast cancer presentation and diagnostic delays in young women. Cancer 2014;120:20-5. [PubMed]
- Poum A, Promthet S, Duffy SW, et al. Factors associated with delayed diagnosis of breast cancer in northeast Thailand. J Epidemiol 2014;24:102-8. [PubMed]
- Gullatte MM, Brawley O, Kinney A, et al. Religiosity, spirituality, and cancer fatalism beliefs on delay in breast cancer diagnosis in African American women. J Relig Health 2010;49:62-72. [PubMed]