
Comparison of the short-term and long-term outcomes of laparoscopic hysterectomies and of abdominal hysterectomies: a case study of 4,895 patients in the Guangxi Zhuang Autonomous Region, China
Introduction
Currently, hysterectomy is one of the most frequently performed operations worldwide. Nine of every ten hysterectomies are performed for benign diseases that negatively affect quality of life (QoL). Total abdominal hysterectomy (TAH) is an accepted, effective and relatively simple treatment that can be performed by general gynecologists. However, TAH is a highly invasive procedure that is associated with morbidity and obviously scars. Since its introduction in the 1940s, laparoscopic surgery has played an important role in gynecology and has several benefits relative to traditional abdominal techniques (1).
Laparoscopy has proven to be a minimally invasive surgical option for patients undergoing hysterectomy. A recent Cochrane review of 47 randomized controlled trials with 5,102 patients (2) that compared different hysterectomy techniques for benign gynecologic diseases reported that patients who undergo laparoscopic hysterectomy (LH) have significantly lower mean blood loss, significantly fewer infections and faster returns to normal activities compared with those who undergo to laparotomy. In contrast, LH has been associated with high rates of complications, particularly urinary tract injuries, compared with abdominal hysterectomy (AH) (OR, 2.61, 95% CI, 1.22-5.60) (3). However, recently published data from a series of 3,190 LHs for benign uterine diseases from Donnez et al. (4) clearly demonstrated that this technique is a safe alternative that is not associated with any increase in major complications when applied by experienced surgeons. Pandit et al. (5) and Driessen et al. (6) concluded that LH is a safe, reproducible technique that is associated with a low complication rate.
There are a great number of reports about the short-term outcomes of both LH and AH, but few studies have reported on long-term QoL outcomes after surgery, including pelvic floor function and sexual function. In the present study, we investigated a series of 4,895 hysterectomies (LH and AH) for benign gynecologic diseases that were performed in 23 third-grade class-A communal hospitals in the Guangxi Zhuang Autonomous Region from January 2007 to December 2013. That is, both the short-term and long-term QoL outcomes were assessed using the International Consultation on Incontinence Questionnaire Lower Urinary Tract (ICIQ-FLUTS) and the Female Sexual Functioning Index (FSFI). Knowledge concerning these outcomes might aid both patients and doctors in making appropriate decisions before surgery.
Methods
Data from the specified database system were analyzed. This database system was researched and developed with Information form the Centre of Guangxi Medical University, which contains measures of gynecologic healthcare quality and resource utilization in the Guangxi Zhuang Autonomous Region. Inpatient data from 23 third-grade class-A communal hospitals throughout the Guangxi Province that began to utilize LH technology in the same era were included in this retrospective study. The quality of the data recorded was ensured by a two-step control system. First, the completeness and exactness of all data were verified within research group by a data controller and double-checked by a senior gynecologist. Second, the data were sent to the central registry of the Guangxi Medical University study group where the accuracy of all data entered in the database was assessed again by the data center quality control group. In cases of discrepancies, the data were returned for verification and correction.
The data from 3,539 patients who underwent LH including total LH [International Classification of Diseases, 9th Revision (ICD-9) 68.41] and laparoscopically assisted vaginal hysterectomy (ICD-9 68.51) between January 2007 and December 2013 were analyzed. These data were compared with data from 1,356 control patients who underwent AH within the same period. Patients with diagnoses of gynecologic malignancies and those who had undergone vaginal or radical hysterectomy were excluded from the analysis. The indications for surgery included myoma uteri, adenomyosis, dysfunctional uterine bleeding (DUB), cervical intraepithelial neoplasia grade Ⅲ (CIN3), endometrial hyperplasia and were recorded for each patient.
The patients’ were assessed in terms of the following variables: demographic characteristics [age, gravidity, parity, and body mass index (BMI)]; medical comorbidities; prior cesarean deliveries; previously abdominal surgeries; indications for the procedure; operative variables as determined from the operative report, including operative time (OT) (defined as the time from skin incision to skin closure), estimated blood loss (EBL), need for blood transfusion, intra- and post-operative complications; surgical pathologic data; passing flatus; days with indwelling catheter; questionnaires covering pelvic floor function (ICIQ-FLUTS) and sexual function (FSFI). Written informed consent was obtained from all patients. The choice of the operative procedure (AH or LH) was based on the patient’s preferences after a thorough discussion of the risks and benefits of each procedure.
The complications were categorized according to time of their detection as intra-operative or post-operative (7).
The intra-operative complications were classified as follows:
(Ⅰ) Serious subcutaneous emphysema;
(Ⅱ) Air embolism;
(Ⅲ) Hemorrhage ≥800 mL;
(Ⅳ) Bladder, ureter or bowel injuries;
(Ⅴ) Vascular injuries (epigastric vessels and major vessels such as the aorta, vena cava or iliac vessels);
(Ⅵ) Other complications resulting in additional procedures or treatments during surgery.
The post-operative complications were classified as follows:
(Ⅰ) Abdominal (or vaginal stump) bleeding or hematoma;
(Ⅱ) Wound infection (defined by the requirement for antibiotic treatment or drainage);
(Ⅲ) Urinary retention;
(Ⅳ) Urinary tract infection (UTI) (defined as a single bacterial growth exceeding 105/mL);
(Ⅴ) Febrile event (defined as a clinically relevant fever of unknown cause with axillary temperature ≥38 ℃ for two consecutive days excluding the first 24 or 48 hours);
(Ⅵ) Deep vein thrombosis (DVT);
(Ⅶ) Pulmonary embolism (PE);
(Ⅷ) Ileus;
(Ⅸ) Other complications.
The causes of each re-operation were recorded. Post-operatively detected organ injuries (i.e., bladder, ureter or bowel) were handled as post-operative complications. Data about the need for and duration of re-admittance to the hospital, re-operations and other types of treatment were collected.
AH is defined as an AH with a 10-cm to 15-cm vertical incision in the abdominal wall, through which the standard operation is carried out (8). All laparoscopic procedures were performed in a modified lithotomy position using a video-monitor to record the laparoscopic part of the operation (including LAVH and TLH). The cup-type uterine manipulator was positioned. The 10-mm laparoscope was introduced through the umbilicus, and 3 accessory 5-mm trocars were introduced suprapubically. The round and utero-ovarian ligaments with the fallopian tubes were diathermy and cut when the adnexa were to be preserved, while the round and infundibulo-pelvic ligaments were diathermy and cut when the adnexa were to be removed. The uterovesical fold of the peritoneum was divided by scissors. The uterine artery and the partial cardinal and uterosacral ligament were diathermy and cut. The cervix was circumcised and the pouch of Douglas opened to allow ligation and division of the partial cardinal and uterosacral ligament, as in a traditional vagina hysterectomy in LVAH. However, all the procedure is performed with laparoscopic techniques and no vaginal surgery is employed in TLH (9).
The LH and AH were performed by surgeons who had conducted each procedure more than 30 times. All surgeries were performed with the patients under general anesthesia, and all patients received preoperative intravenous prophylactic antibiotics. A Foley catheter was is inserted during surgery to empty the bladder. Carbon dioxide pneumoperitoneum was achieved using a Veres needle and a pressure not higher than 15 mmHg. Four laparoscopic disposable ports, including the umbilicus, were used.
The International Consultation on Incontinence Questionnaire Female Lower Urinary Tract (ICIQ-FLUTS) is a 12-item questionnaire that was derived from the Bristol Female Lower Urinary tract questionnaire and measures female lower urinary tract symptoms and symptom bothersomeness (urinary-related QoL), with 0 being no symptoms and 48 being severe overall filling/voiding/incontinence symptoms. Bother of each symptom is measured on a Likert scale of 0 (not at all) to 10 (a great deal). According to the degree of stress urinary incontinence (SUI) in ICIQ-FLUTS questionnaire score standard, symptoms occurred in the past 4 weeks less than 10 days (1 point) is mild SUI, 10-20 days (2 points) is moderate SUI, more than 20 days (3 points) is severely SUI, every day is serious SUI (10). This questionnaire has been validated in Chinese dialects (11, 12). Patients were evaluated pre-operation (baseline) and 12 months after surgery.
Sexual functions of the study participants were also assessed with the FSFI twice (baseline and 12 months after surgery. This questionnaire has been validated in Chinese dialects too (13, 14). The survey is a brief, anonymous multi-dimensional, questionnaire that is used to assess sexual function via its 19 questions (15). The questions were grouped and scored for the domains of sexual desire (two questions), arousal (four questions), lubrication (four questions), orgasm (three questions), satisfaction (three questions), and pain during sexual intercourse (three questions). These factors were 0.6 for desire, 0.3 for arousal and lubrication, and 0.4 for orgasm, satisfaction, and pain. Total score was obtained by adding the six domain scores and was calculated multiplying the sum by the factors in domain. Therefore, total the FSFI score range was 2-36. A total score of 26.55 or less is suggestive of female sexual dysfunction (FSD) (16).
Letters of introduction describing the nature of the study and questionnaires were mailed to eligible patients and controls and asked for their participation. The letter also stated that a project interviewer would additionally contact eligible women by phone or e-mail to provide support to those who had experienced difficulty completing the questionnaires.
All data are presented as the means ± the standard deviations (SDs) and medians (ranges) for continuous variables and categorical variables as the numbers of cases (n) and percentages of occurrence (%). All hypothesis tests were conducted using a P value of 0.05 for statistical significance. Between-group differences in categorical data were analyzed with chi-square tests and Fisher’s exact tests. All statistical analyses were performed using the Statistical Package for the Social Sciences (SPSS, version 18.0 for Windows; SPSS, Inc., Chicago, Illinois, USA).
Results
Briefly, 4,895 hysterectomies were reported; among these, 1,356 were performed via the TAH procedure, and 3,539 were performed via the laparoscopic approach (1,547 LVAH and 1,992 TLH based on uterus volume, which did not exceed that of 8 weeks’ pregnancy). All of the patients’ demographic and clinical characteristics, including age, BMI, uterine size, medical comorbidities, previous abdominal surgeries, prior cesarean deliveries and indications for the procedure are displayed in Table 1. The average ages were 46.7±6.1 (LH) and 46.8±6.6 (AH) years. The average body mass indices were 23.4±3.2 (LH) and 23.9±2.9 (AH) kg/m2. The uterine size, prior cesarean delivery, previous abdominal surgeries, medical comorbidities and indications for surgery did not differ significantly between groups. Myoma uteri, adenomyosis, DUB, CIN3, and endometrial hyperplasia accounted for the majority of the indications for surgery.

Full table
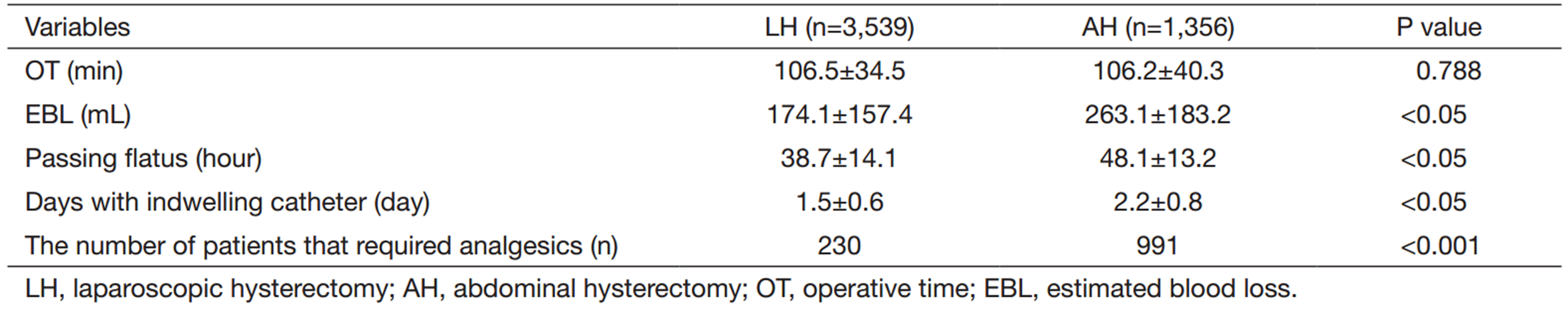
Table 2 provides details about the operative and postoperative variables for the LH and AH groups. The EBL (174.1±157.4 vs. 263.1±183.2 mL in the LH and AH groups, respectively), passing flatus (38.7±14.1 vs. 48.1±13.2 hours), days with indwelling catheter (1.5±0.6 vs. 2.2±0.8 days), use of analgesics [230 (6.5%) vs. 991 (73.1%)] of the LH group were significantly lower than those of the AH group. There was no significant difference in OT (106.5±34.5 vs. 106.2±40.3 min) between the two groups.
Full table
The intra- and post-operative complications are detailed in Table 3. The all-type intra-operative complication rate of the LH group [2.4% (85 cases)] was significantly less that of the AH group [4.1% (56 cases)]. Similarly, the all-type post-operative complication rate of the LH group [2.3% (81 cases)] was significantly less than that of the AH group [5.7% (77 cases)].

Full table
The pelvic floor and sexual functional questionnaire scores of the two groups of patients are shown in Tables 4-6. Among the 4,895 women who we attempted to contact via the mail or telephone, 3,380 (95.5%) in LH group and 1,305 (96.2%) in the AH group returned the questionnaire to us. The reasons for patient exclusion included the following: incomplete questionnaires, no sexual activity over the last 4 weeks due to a husband’s business trip or widowhood, and a lack written informed consent.

Full table

Full table

Full table
Among the patients who responded to the ICIQ-FLUTS questionnaire, there was no significant difference between two groups in from mild to serious SUI in 12 months after surgery and pre-operation (baseline) (P>0.05, Table 4). In addition, the proportion of patients who experienced constipation in the LH group [12.1% (409 cases)] was significantly lower than that of in the AH group [24.6% (321 cases; P=0.002].
Tables 5 and 6 show the FSFI domain scores and total scores for each group based on the patient reports. Lubrication and satisfaction domain scores for the LH group were significantly elevated compared with the AH group 12 months after surgery (P<0.001). However, there was no significant difference between two groups in the other four domain scores (P>0.05, Table 5). Additionally, based on the FSFI total score optimal cut-off of 26.55 for differentiating the women with and without sexual dysfunction, the benefit of LH group versus AH group was less proportion of women with sexual dysfunction (FSFI total score <26.55) 12 months after surgery compare to baseline (P<0.01, Table 6).
Discussion
Since the first LH was described by Reich et al. in 1989 (17), the laparoscopic approach has become the approach of choice for gynecological surgery. LH has been proven to cause less pain and shorten recovery time compared to laparotomy (18). Given the retrospective nature of this study, the absence of randomization, and the variability in the length of the postoperative observation period, the interpretation and informative values of some of the parameters is limited. However, the present multi-center, retrospective, exploratory cohort study is currently the largest report that compares two different methods of hysterectomy within the same time-period in the world. The patients were matched in terms of age, BMI, uterine size, and medical comorbidities. Previously abdominal surgeries, prior cesarean deliveries and the indications for the procedures were not significantly different between the groups.
The first stages of TLH and LAVH require OTs of approximately 100-240 minutes, which are long compared to TAH (19, 20). Nevertheless, there was no significant difference in OT between the two groups in our study because the data were obtained from 23 third-grade class-A communal hospitals in 2007-2013, and LH techniques in the Guangxi Province had improved by that time. Similarly, advanced laparoscopic devices, such as the Ligasure or Plasma Kinetic System (PKS), are able to stop bleeding by coagulation and cut tissues at the same time, which is safe, efficient and time-saving. Furthermore, our analysis also suggested that the LH groups experienced less blood loss, shorter passing flatus, fewer days with indwelling catheter and less pain. These findings are in keeping with additional publications (21, 22). These results might be due to the more precise and accurate anatomical location, improved visualization of the deep vascular structures and reduced tissue trauma that are enabled by laparoscopic surgery.
Regarding intra- and post-operative complications, our results differ from those in the literature, particularly in terms of the risk of urinary tract injuries. Some authors have observed a higher incidence of urinary tract injuries with laparoscopic than with AH (23). Janssen et al. (24) analyzed all known ureter injuries that had occurred during LH for benign indications in the Netherlands to identify the patient-related and surgeon-related risk factors. The authors concluded that insufficient training and inadequate application of techniques, such as coagulation of the uterine artery without the use of a uterine manipulator could be considered to be the main predisposing factors. Lgwe et al. (25) investigated the effects of resident involvement on the morbidity of patients following total LH for benign disease. The results showed that in cases with resident involvement the probability of the administration of postoperative blood transfusion [odds ratio (OR), 4.98; 95% confidence interval (CI), 2.18-11.33], reoperation (OR, 1.7, 95% CI, 1.01-2.89) and readmission (OR, 1.93, 95% CI, 1.09-3.42) was increased. Mitri et al. (26) reported on 434 patients who had undergone underwent hysterectomy for benign disease. He found that the median OT was 86 minutes, the median blood loss was 95 mL, and the median hospital stay was 1 day. In our study, total intra-operative complication rates of 2.4% (n=85) and 4.1% (n=56) were observed for LH and TAH, respectively. The complication rates following laparoscopic and AH were 2.3% (n=81) and 5.7% (n=77), respectively. LH performed better than TAH presumably because from 2007 to 2013, 3,539 laparoscopic hysterectomies were performed by the experienced laparoscopists, which resulted in an average of 100 laparoscopic hysterectomies per year by the same surgical team. Moreover, we combined the use of a cup-type uterine manipulator with advanced laparoscopic instruments (Ligasure or PKS) in the laparoscopic hysterectomies. The cup-type uterine manipulator sets the cervix and vaginal fornix close to the cup, and the bladder is easily separated from the former cervix and vagina, which might have reduced the risk of bladder injury. Additionally, the lateral vaginal vault was moved up, so the upper vagina was stretched, and the distance of the uterine blood vessels from the ureter was increased to avoid damage.
Pelvic floor dysfunction describes a range of problems associated with one or more of the three systems in the pelvic floor, i.e., the urinary system, anorectal system, and genital system. In addition to the short-term outcomes during surgery, we also evaluated the long-term QoL outcomes (as assessed with the ICIQ-FLUTS and FSFI) following the LH and TAH operations. Regardless of the type of hysterectomy, not only can cutting and mechanical stress can cause muscle damage directly, but in addition reduction in the level of neurotransmitters that reach the pelvic blood vessels can also result in insufficient blood perfusion and cause muscle atrophy and degeneration (27). Defecation and urination are controlled by the pudendal and splanchnic nerves, and damage to the intra-operative muscle, connective tissue, blood vessels and nerves can lead to spatial structure changes in the pelvis. Increase of abdominal pressure can also cause post-operative urinary incontinence and bowel disorders (28). Moreover, sexual function requires normal nerve reflex function, anatomical structures, blood supply and mental state (29). The pelvic floor support structure is damaged after hysterectomy, and vaginal fornix shortening can cause sexual difficulties. The destruction of the uterus and vaginal plexus causes changes in sexual feelings (30). The pelvic autonomic nerve is damaged, which alters the blood supply to the vaginal wall and vaginal lubrication and can cause changes in hormone levels that causing premature ovarian aging and other clinical problems (31). In our study, there was no significant difference between the two groups in from mild to serious SUI in 12 months after surgery and pre-operation (baseline) (P>0.05). The proportion of patients who experienced constipation in the LH group was significantly lower than that in the AH group (P=0.002). Lubrication and satisfaction domain scores in FSFI for the LH group were significantly higher in comparison to the AH group 12 months after surgery (P<0.001), no significant difference between the two groups in the other four domain scores (P>0.05) was observed. The benefit of the LH group versus the AH group was smaller in the proportion of women with sexual dysfunction 12 months after surgery compared to baseline (P<0.001). These findings are in agreement with those reported elsewhere in the literature (27, 32). For example, Kluivers et al. (33) assessed and compared the incidence of urinary incontinence, bowel dysfunction, and sexual problems following LH and AH in a randomized controlled trial. Prior to and 3 months after the surgery patients were asked if they experienced urinary incontinence and requested to complete the validated Urogenital Distress Inventory, Incontinence Impact Questionnaire, Defecatory Distress Inventory, and Questionnaire for Screening Sexual Dysfunctions 1 year after surgery. The results suggested that the incidence of urinary incontinence in the 3 months following surgery had decreased similarly in both groups compared to baseline. Urinary incontinence and sexual problems were rare. One year after surgery, a significant treatment effect favoring LH was observed in the results of the Urogenital Distress Inventory and Incontinence Impact Questionnaire, whereas no difference was observed in the Defecatory Distress Inventory or Questionnaire for Screening Sexual Dysfunctions. Ayoubi et al. (34) analyzed the effect on sexual functioning that followed trans-vaginal, laparoscopic and abdominal hysterectomies. These authors found that sexual damage occurred in 24%, 13.5% and 8.5% of the abdominal, vaginal, and laparoscopic surgery, respectively.
In conclusion, the present retrospective study demonstrated LH being a safe and effective treatment of benign gynecological disease and is also capable to improve patients’ QoL in the long-term. However, with increasing numbers of surgical indications, the complication rate will gradually rise. It is important for us to reduce the rate of complications by strengthening the surgeons’ training in laparoscopic skills, increase their learning, improve laparoscopic surgical instruments, and choose the indications carefully. The decision about the surgical approach to hysterectomy should be made by the patient based on discussions with her surgeon about the relative benefits and hazards. These benefits and hazards seem to depend primarily on surgical expertise and this might influence the decision. Furthermore, well-designed multi-center studies that focus on the long-term QoL following LH are warranted before definite conclusions can be drawn.
Acknowledgements
We express our gratitude to the director of Guangxi Medical University Information Centre Professor Zhong Tang and his assistant MD Xu Ou. We also wish to thank student volunteers Jing Huang, Xiaoyun Gao and Dandan Chen for their assistance with questionnaire survey; Xiaomin Yang, Jie Lin and Wenwen Zhang for their major role in accomplishing the data entry. Finally, this study would not have been possible without the participants, and we extend our gratitude to these many individuals.
Footnote
Conflicts of Interest: The authors have no conflicts of interest to declare.
References
- Németh G. Indications and methods of hysterectomy. Orv Hetil 2014;155:1152-7. [PubMed]
- Aarts JW, Nieboer TE, Johnson N, et al. Surgical approach to hysterectomy for benign gynaecological disease. Cochrane Database Syst Rev 2015;8:CD003677. [PubMed]
- Nieboer TE, Johnson N, Lethaby A, et al. Surgical approach to hysterectomy for benign gynaecological disease. Cochrane Database Syst Rev 2009:CD003677. [PubMed]
- Donnez O, Jadoul P, Squifflet J, et al. A series of 3190 laparoscopic hysterectomies for benign disease from 1990 to 2006: evaluation of complications compared with vaginal and abdominal procedures. BJOG 2009;116:492-500. [PubMed]
- Pandit MJ, Alsop R. Using international data to set benchmarks for morbidity outcomes after hysterectomy. Int J Gynaecol Obstet 2016;133:84-8. [PubMed]
- Driessen SR, Sandberg EM, van den Haak L, et al. Increase in laparoscopic hysterectomy: shift in indications and dilemmas. Ned Tijdschr Geneeskd 2015;159:A9324. [PubMed]
- Brummer TH, Jalkanen J, Fraser J, et al. FINHYST, a prospective study of 5279 hysterectomies: complications and their risk factors. Hum Reprod 2011;26:1741-51. [PubMed]
- Sutton C. Past, present, and future of hysterectomy. J Minim Invasive Gynecol 2010;17:421-35. [PubMed]
- Papadopoulos MS, Tolikas AC, Miliaras DE. Hysterectomy-current methods and alternatives for benign indications. Obstet Gynecol Int 2010;2010. pii: 356740. [PubMed]
- Hilton P, Armstrong N, Brennand C, et al. A mixed methods study to assess the feasibility of a randomised controlled trial of invasive urodynamic testing versus clinical assessment and non-invasive tests prior to surgery for stress urinary incontinence in women: the INVESTIGATE-I study. Trials 2015;16:400. [PubMed]
- Ge J, Lu Y, Zhang Y, et al. The prevalence and cognition of urinary incontinence among female adults in Beijing. Chinese Journal of Clinical Obstetrics and Gynacology 2010;11:15-17.
- Wang D, Wang Y, Xu K, et al. Prevalence of lower urinary tract symptoms in non-urological outpatients treated in Peoples’ Hospital of Peking University. Journal of Modern Urology 2013;18:457-60.
- Lou Q, Zhang Q, Yao H, et al. Translation of Female Sexual Function Index (FSFI) into Chinese and its reliability and validity evaluation. Chinese Journal of Practical Nursing 2013;29:23-6.
- Shi YF, Shao XY, Lou QQ, et al. Study on female sexual dysfunction in type 2 diabetic Chinese women. Biomed Environ Sci 2012;25:557-61. [PubMed]
- Rehman KU, Asif Mahmood M, Sheikh SS, et al. The Female Sexual Function Index (FSFI): Translation, Validation, and Cross-Cultural Adaptation of an Urdu Version "FSFI-U". Sex Med 2015;3:244-50. [PubMed]
- Tungmunsakulchai R, Chaikittisilpa S, Snabboon T, et al. Effectiveness of a low dose testosterone undecanoate to improve sexual function in postmenopausal women. BMC Womens Health 2015;15:113. [PubMed]
- Reich H, DeCaprio J, McFlynn F. Laparoscopic hysterectomy. J Gynecol Surg 1989;5:213-6.
- Dall'Asta A, Patrelli TS, Franchi L, et al. Total laparoscopic hysterectomy: our experience from 2008 to 2012. Ann Ital Chir 2013;84:645-8. [PubMed]
- Ridgeway BM, Buechel M, Nutter B, et al. Minimally Invasive Hysterectomy: An Analysis of Different Techniques. Clin Obstet Gynecol 2015;58:732-9. [PubMed]
- Drahonovsky J, Haakova L, Otcenasek M, et al. A prospective randomized comparison of vaginal hysterectomy, laparoscopically assisted vaginal hysterectomy, and total laparoscopic hysterectomy in women with benign uterine disease. Eur J Obstet Gynecol Reprod Biol 2010;148:172-6. [PubMed]
- Oksuzoglu A, Seckin B, Turkcapar AF, et al. Comparison of tissue trauma after abdominal, vaginal and total laparoscopic hysterectomy. Ginekol Pol;86:268-73.
- Sutasanasuang S. Laparoscopic hysterectomy versus total abdominal hysterectomy: a retrospective comparative study. J Med Assoc Thai 2011;94:8-16. [PubMed]
- Dassel MW, Adelman MR, Sharp HT. Recognition and Management of Urologic Injuries With Laparoscopic Hysterectomy. Clin Obstet Gynecol 2015;58:805-11. [PubMed]
- Janssen PF, Brölmann HA, Huirne JA. Causes and prevention of laparoscopic ureter injuries: an analysis of 31 cases during laparoscopic hysterectomy in the Netherlands. Surg Endosc 2013;27:946-56. [PubMed]
- Igwe E, Hernandez E, Rose S. Resident participation in laparoscopic hysterectomy: impact of trainee involvement on operative times and surgical outcomes. Am J Obstet Gynecol 2014;211:484.e1-7. [PubMed]
- Mitri M, Fanning J, Davies M, et al. Minimally invasive hysterectomy at a university teaching hospital. JSLS 2014;18.
- Radosa JC, Meyberg-Solomayer G, Kastl C, et al. Influences of different hysterectomy techniques on patients' postoperative sexual function and quality of life. J Sex Med 2014;11:2342-50. [PubMed]
- Ercan Ö, Özer A, Köstü B, et al. Comparison of postoperative vaginal length and sexual function after abdominal, vaginal, and laparoscopic hysterectomy. Int J Gynaecol Obstet 2016;132:39-41. [PubMed]
- Goktas SB, Gun I, Yildiz T, et al. The effect of total hysterectomy on sexual function and depression. Pak J Med Sci 2015;31:700-5. [PubMed]
- Lonnée-Hoffmann R, Pinas I. Effects of Hysterectomy on Sexual Function. Curr Sex Health Rep 2014;6:244-51. [PubMed]
- Fram KM, Saleh SS, Sumrein IA. Sexuality after hysterectomy at University of Jordan Hospital: a teaching hospital experience. Arch Gynecol Obstet 2013;287:703-8. [PubMed]
- Rodríguez MC, Chedraui P, Schwager G, et al. Assessment of sexuality after hysterectomy using the Female Sexual Function Index. J Obstet Gynaecol 2012;32:180-4. [PubMed]
- Kluivers KB, Mol BW, Bremer GL, et al. Pelvic organ function in randomized patients undergoing laparoscopic or abdominal hysterectomy. J Minim Invasive Gynecol 2007;14:442-8. [PubMed]
- Ayoubi JM, Fanchin R, Monrozies X, et al. Respective consequences of abdominal, vaginal, and laparoscopic hysterectomies on women's sexuality. Eur J Obstet Gynecol Reprod Biol 2003;111:179-82. [PubMed]