
Epidemiology and trend analysis on malignant mesothelioma in China
Introduction
Malignant mesothelioma, a rare cancer, is highly correlated with asbestos exposure. The latency period from exposure to disease-related risk factors and clinical symptoms were about 20–40 years (1). According to the cancer site, the disease comprises two major types, pleural and peritoneal mesothelioma. Researches identified that knowledge gaps are barriers to preventing and treating malignant mesothelioma (2). In China, few researches reported on malignant mesothelioma incidence and mortality situation. In this study, we use the most update data from National Central Cancer Registry (NCCR) to analyze the malignant mesothelioma epidemiology and its trend, and the results would help health-related staff to know more about this disease and provide basic information for policy-makers.
Materials and methods
Data source
The NCCR is in charge of population-based cancer registry with responsibility of data collection, evaluation and publication from local cancer registries in China (3). By 1st June 2016, 347 cancer registries (126 cities and 221 counties) from 32 provinces submitted 2013 data to the NCCR. After quality control, 255 cancer registries (88 cities and 167 counties) meet the requirements. Data covered about 226,494,490 people (114,860,339 males and 111,634,151 females), accounting for about 16.65% of the national population at the end of 2013. Invasive cases of malignant mesothelioma (ICD10: C45) were extracted and analyzed from the overall cancer database.
Population data
We use the fifth and the sixth National Population Census data provided by the National Statistics Bureau of China to estimate the national population in 2013, taking into account changes in age structure, gender ratio, and the proportion of urban and rural transformation released by the National Bureau of Statistics (http://data.stats.gov.cn/). The 2013 national population was stratified by area (urban/rural), gender, and 19 age groups (0–, 1–4, 5–84 by 5 years, 85+ years). Changes in age-specific death probability were also adjusted when calculating the population. Linear changes were assumed in each age group between the fifth and sixth population censuses.
Quality control
Data submitted to the NCCR were evaluated according to “Guideline for Chinese Cancer Registration” (4) and referring to relevant data quality criterion of “Cancer Incidence in Five Continents Volume IX” by International Agency for Research on Cancer/International Association of Cancer Registries (IARC/IACR) (5). The percentage of morphological verification (MV%), the percentage of death certificate-only cases (DCO%), mortality to incidence (M/I) ratio, and the percentage of unknown basis of diagnosis (UB%) were used to evaluate the completeness, validity and reliability of cancer statistics (6,7).
Statistical analysis
Incidence and mortality, proportions, crude, age-standardized, accumulated, truncated, and age-specific incidence and mortality rates were calculated by area, gender and age groups. The number of new cases and deaths were estimated using the 5-year age-specific cancer incidence/mortality rates and the corresponding populations. The Chinese population in 2000 and Segi’s world population were used to calculate age-standardized rates. The cumulative risk of developing or dying from cancer before 75 years of age (in the absence of competing causes of death) was calculated and presented as a percentage. Truncated age-standardized rate was calculated among the cases aged between 35 and 64 years old. Software including MS-Excel, IARCcrgTools 2.05 issued by IARC/IACR were used for data checking and evaluation. SAS (version 9.2; SAS Institute, Cary, NC, USA) was used to calculate incidence and mortality rates. Trend analysis were conducted using Joinpoint Regression Program 3.4.3 software (Version 3.4.3; National Cancer Institute, USA) (8). Linear model was used to calculate the crude and age-standardized rates of annual percentage change (APC) and its 95% confidential interval (95% CI).
Results
Data quality
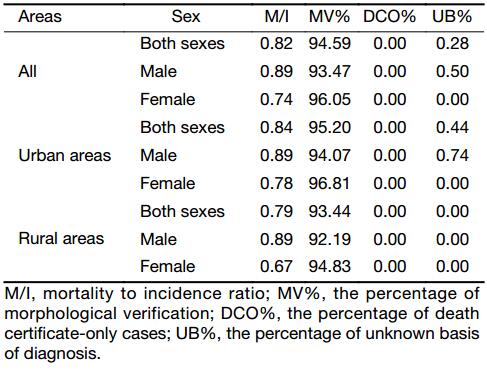
There were 255 qualified cancer registries included in the final analysis. The data quality indicators of MV%, DCO%, M/I and UB% were 94.59%, 0.00%, 0.82 and 0.28, respectively. In urban areas, they were 95.20%, 0.00%, 0.84 and 0.44, respectively. In rural areas, they were 93.44%, 0.00%, 0.79 and 0.00, respectively (Table 1).
Full table
Incidence
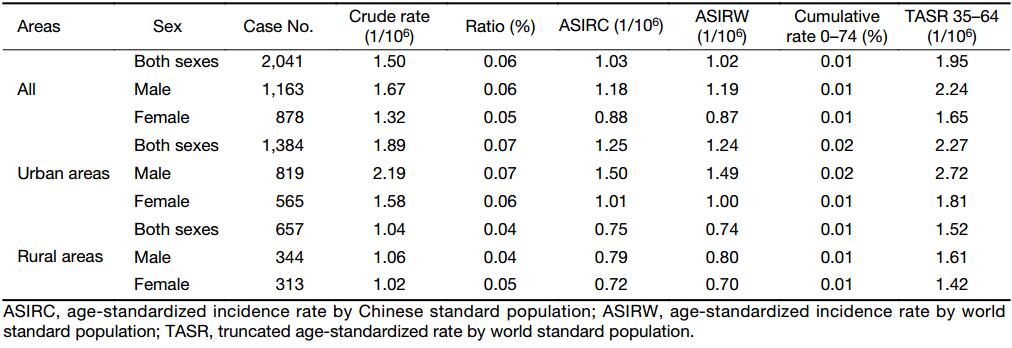
There was an estimated of 2,041 new malignant mesothelioma cases occurred in China in 2013, accounting for 0.06% of all new cancer cases. The crude incidence, age-standardized rate of incidence by Chinese standard population (ASIRC), and age-standardized rate of incidence by world standard population (ASIRW) of breast cancer were 1.50/106, 1.03/106, and 1.02/106, respectively. In patients aged 0–74 years, the cumulative incidence rate was 0.01%, while for those aged 35–64 years, the truncated age-standardized rate (TASR) was 1.95/106 (Table 2).
Full table
The estimated number of new malignant mesothelioma cases in urban areas in 2013 was about 1,384, accounting for 0.07% of all new cancer cases. The crude incidence, ASIRC and ASIRW in urban areas were 1.89/106, 1.25/106 and 1.24/106, respectively. The cumulative incidence rate was 0.02% and the TASR was 2.27/106. The estimated number of new malignant mesothelioma cases in rural areas in 2013 was about 657, accounting for 0.04% of all new cancer cases. The crude incidence, ASIRC and ASIRW in rural areas were 1.04/106, 0.75/106 and 0.74/106, respectively. The cumulative incidence rate was 0.01% and the TASR was 1.52/106. The incidence rate was higher in urban than in rural areas (Table 2).
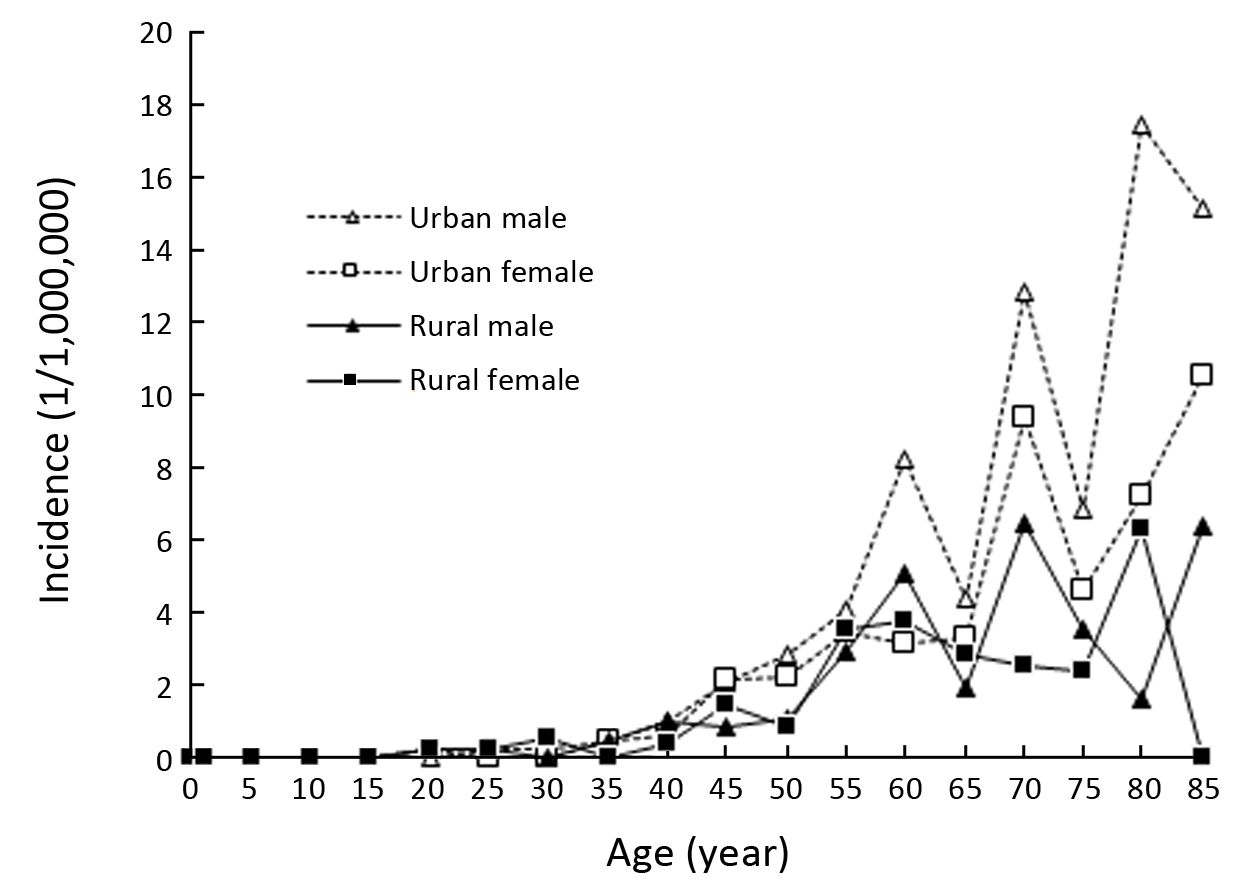
In 2013, the age-specific incidence of malignant mesothelioma was increased after 35 years old with fluctuated incidence rates (Figure 1).
Mortality
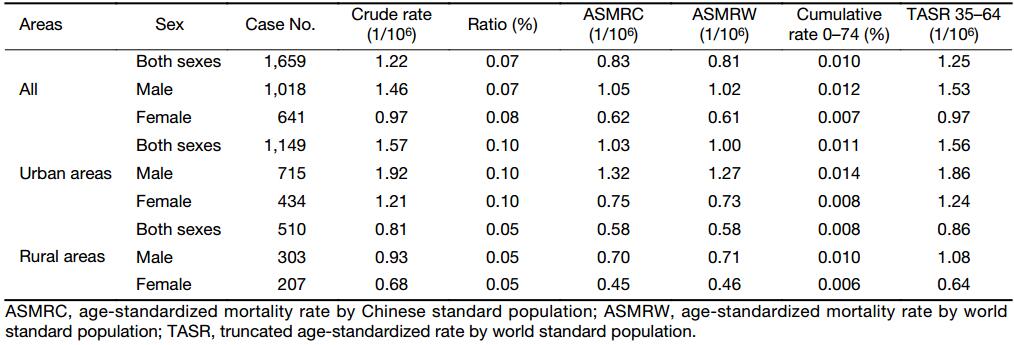
There was an estimated of 1,659 malignant mesothelioma deaths occurred in China in 2013, accounting for 0.07% of all cancer deaths. The crude mortality, age-standardized rate of mortality by Chinese standard population (ASMRC), and age-standardized rate of mortality by world standard population (ASMRW) of breast cancer were 1.22/106, 0.83/106, and 0.81/106, respectively. In patients aged 0–74 years, the cumulative mortality rate was 0.01%, while for those aged 35–64 years, the truncated age-standardized rate (TASR) was 1.25/106 (Table 3).
Full table
The estimated number of malignant mesothelioma deaths in urban areas in 2013 was about 1,149, accounting for 0.10% of all cancer deaths. The crude mortality, ASMRC and ASMRW in urban areas were 1.57/106, 1.03/106 and 1.00/106, respectively. The cumulative mortality rate was 0.01% and the TASR was 1.56/106. The estimated number of malignant mesothelioma deaths in rural areas in 2013 was about 510, accounting for 0.05% of all cancer deaths. The crude mortality, ASMRC and ASMRW in rural areas were 0.81/106, 0.58/106 and 0.58/106, respectively. The cumulative mortality rate was 0.01% and the TASR was 0.86/106. The mortality rate was higher in urban than in rural areas (Table 3).
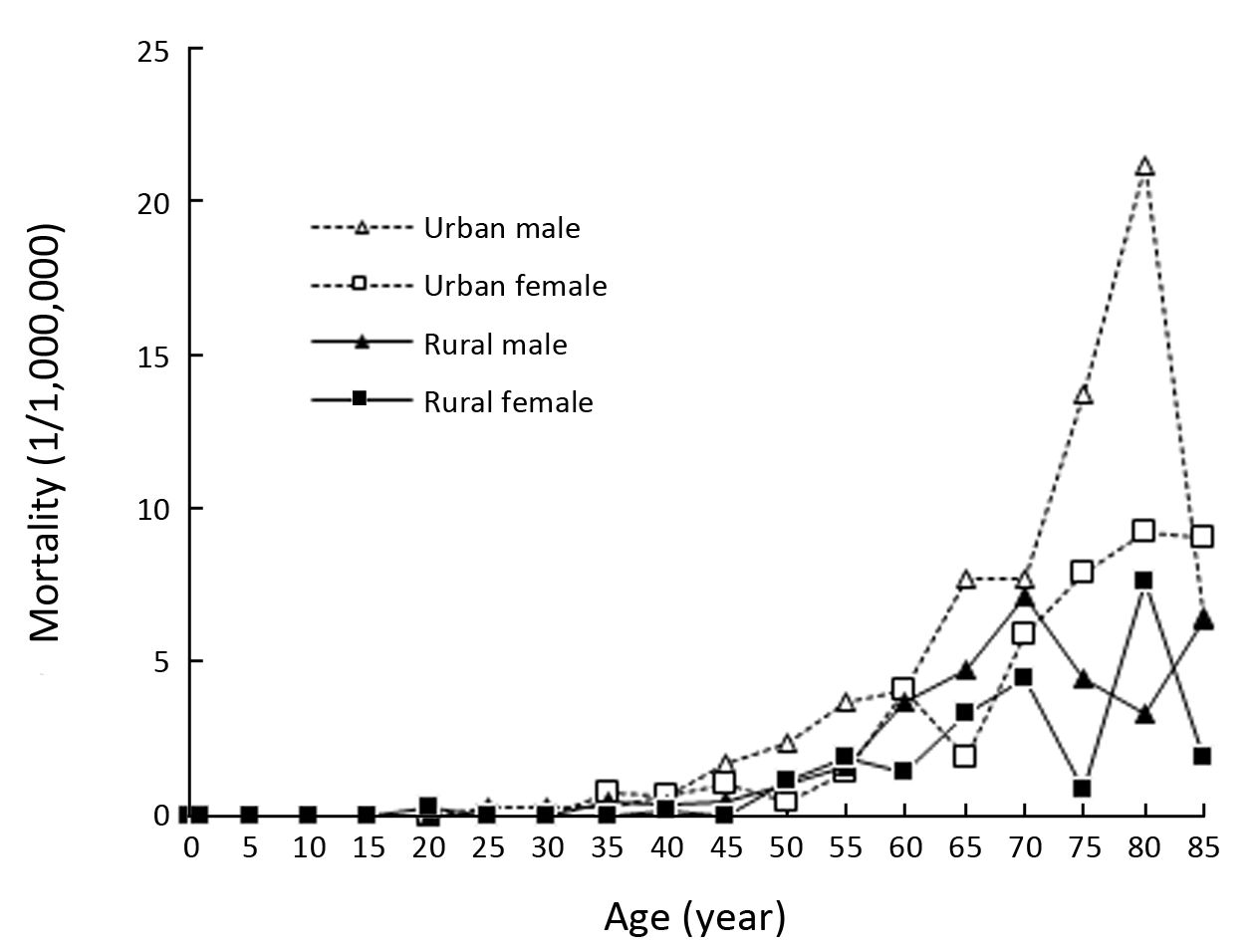
In 2013, the age-specific mortality of malignant mesothelioma was increased after 40 years old with fluctuated mortality rates, and males had higher mortality rates than females (Figure 2).
Trend
Incidence trend
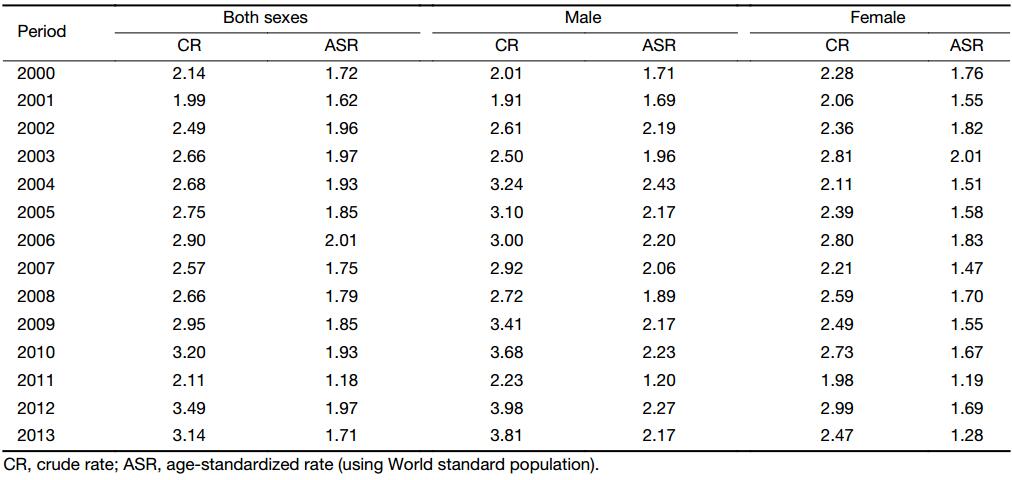
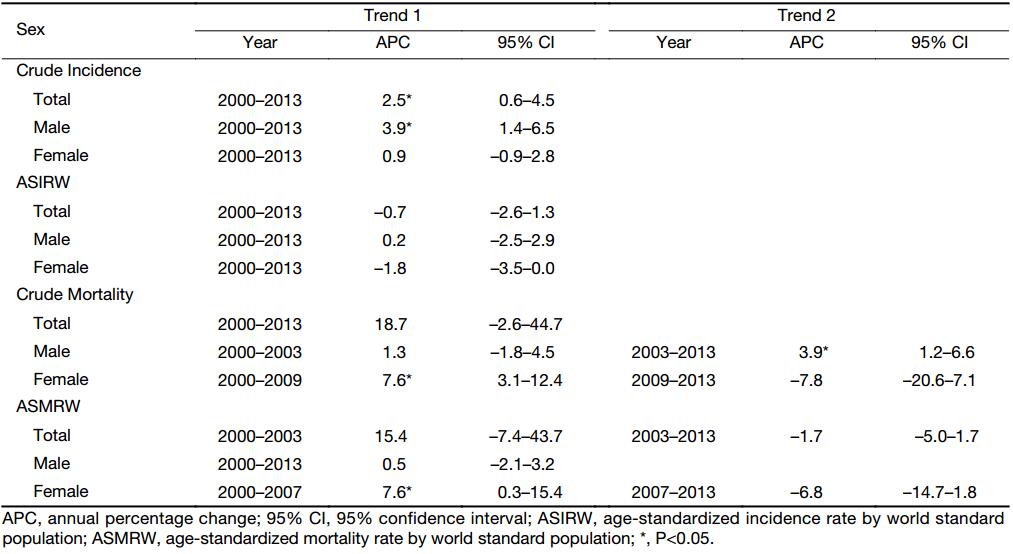
During 2000–2013, the incidence rate of 22 cancer registries was 2.14/106 in 2000 and increased to 3.14/106 in 2013. In males, it increased from 2.01/106 to 3.81//106, while in females, it increased from 2.28/106 to 2.47/106. After age standardization, the incidence rate was 1.72/106 in 2000 and decreased to 1.71/106. It increased from 1.71/106 to 2.17/106 for males, while decreased from 1.76/106 to 1.28/106 for females. The Joinpoint trend analysis showed that there was an increasing trend of incidence rate of malignant mesothelioma in registration areas of China during 2000–2013 with an APC of 2.5% (95% CI: 0.6%–4.5%); the same increasing trend was observed in males with an APC of 3.9% (95% CI: 1.4%–6.5%); and no significant differences were observed in females. After age standardization, no significant differences were observed in both sexes (Table 4, 5).
Full table
Full table
Mortality trend
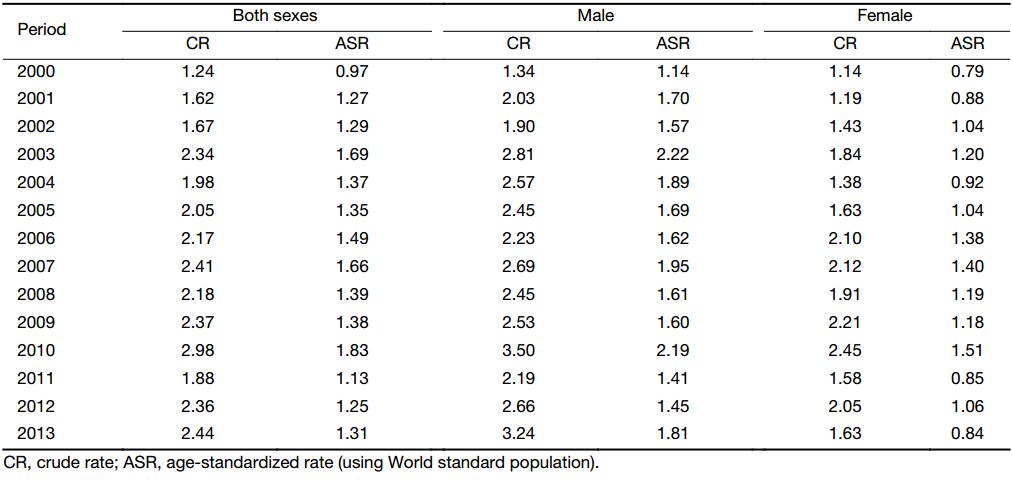
During 2000–2013, the mortality rates of 22 cancer registries increased from 1.24/106 in 2000 to 2.44/106 in 2013. It increased from 1.34/106 to 3.24/106 for males, and for females, it increased from 1.14/106 to 1.63/106. After age standardization, the mortality rate was 0.97/106 in 2000 and increased to 1.31/106. In both sexes, they showed increasing trends. It increased from 1.14/106 in 2000 to 1.81/106 in 2013 in males and 0.79/106 to 0.84/106 in females. The Joinpoint trend analysis showed that no significant differences were observed in both sexes, while an increasing trend of mortality rate was observed in males during 2003–2013 with an APC of 3.9% (95% CI: 1.2%–6.6%). In females, during 2000–2009, we also see an increasing trend with an APC of 7.6% (95% CI: 3.1%–12.4%). After age standardization, no significant differences were observed, except for females during 2000–2007 with an APC of 7.6% (95% CI: 0.3%–15.4%) (Table 5, 6).
Full table
Discussion
Malignant mesothelioma is an environment and occupation-related cancer with poor survival. With the rapid development of Chinese economy, progressing industrialization may result in a series of problems which need to be concerned. Asbestos is an important industrial mineral which can lead to asbestos-related diseases. Malignant mesothelioma is one of major diseases induced by asbestos. Almost all of the asbestos consumption concentrated in developing economies. In 2010, Asian accounted for 60% of the global chrysotile consumption, compared with 30% for China (9). More attention should be attached on monitoring, diagnosis, treatment and registration of malignant mesothelioma and make data regards to its incidence and mortality accessible for researchers.
The incidence or mortality rates varied across the regions of the world. The incidence rates were higher in some European countries (UK, the Netherlands, Malta, Belgium) and some Oceanian countries (Australia, New Zealand), Japan and countries from central Europe had relatively low incidence/mortality rates (10). According to the Surveillance, Epidemiology, and End Results (SEER) Cancer Statistics Review figures, the age-adjusted incidence rate was 0.92/105 in 2014, 1.59/105 in males and 0.42/105 in females. And 5-year relative survival was 9.1% during 2007–2013 (11). In the USA, deaths with malignant mesothelioma were increasing from 2,479 deaths in 1999 to 2,597 in 2015 with age-adjusted death rates decreased from 1.40/105 in 1999 to 1.09/105 in 2015 (12). The UK has been conducting researches on malignant mesothelioma deaths since 1968. According to the latest statistics of the UK, there were 2,515 mesothelioma deaths due to past asbestos exposures in 2014 (13). During 1993–2014, the European age-standardized incidence rates in the UK increased from 5.1/105 to 8.9/105 in males, and from 0.7/105 to 1.3/105 in females (14). In Australia, the ASIRW was 0.9/105 in 1982 and increased to 1.5/105 in 2013, while the ASMRW was 1.5/105 in 1997 and decreased to 1.3/105 in 2014 (12). According to the report from Hong Kong, China, the estimated annual incidence rate was 1.0/106 (15). When compared with western countries, the incidence rate in Eastern Asia is very low (16). The reasons to explain the discrepancy may be complex, such as underdiagnosis or underregistration of malignant mesothelioma, and not developing into malignant tumors for the long latency periods of the disease. Besides, genetic susceptibility, environmental exposures, occupational exposures may play as co-factors in the development of malignant mesothelioma. The incidence and mortality rates in China were relatively low. There is a big concern that most Chinese physicians do not have experience to diagnose the rare disease. Malignant mesothelioma, especially peritoneal malignant mesothelioma, is often misdiagnosed in eastern China (17), and more and more professional training on diagnosis procedure of the disease should be enhanced. The incidence trend of malignant mesothelioma was increasing in China, while its mortality trend was stable. The changes in trend were similar to that of more developed countries.
Malignant tumors are a kind of multi-factor and multi-stage disease, and there are many factors associated with malignant mesothelioma. Occupational asbestos exposure is the major factor in developing the aggressive disease. Workers could exposure to asbestos through a variety of industrial operations, including mining and milling, manufacturing, shipbuilding and repair, and construction (18). In addition, environmental exposure to asbestos could also contribute to malignant mesothelioma, including naturally occurring asbestos exposure, neighborhood or household exposure to occupationally exposed subjects, and one major feature found in this kind of causes was that a higher disease burden was observed in females than in males (19). Asbestos-related diseases are of big threat to lives that result in heavy disease burden. Based on the estimation of National Center for Health Statistics mortality data, during 1999–2010, a total of 427,005 years of potential life lost to life expectancy (YPLL) and 55,184 years of potential life lost to life expectancy to age 65 (YPLL65) were attributed to asbestosis (56,907 YPLL and 2,167 YPLL65) and malignant mesothelioma (370,098 YPLL and 53,017 YPLL65) (20).
This study provided the latest data on the epidemiology of malignant mesothelioma and further analyzed its trends in China. The results will be helpful in deep understand of the current situation of malignant mesothelioma and provide basic information for health-related staff to monitor and control the disease. Although the incidence or mortality rate of malignant mesothelioma in China was relatively low compared with western countries, the incidence rate of malignant mesothelioma showed an increasing trend which should be paid more attention. Therefore, strengthening supervision laws to restricted asbestos use and further enhancing primary and secondary prevention of high risk subjects would be put in the first place.
Acknowledgements
We gratefully acknowledged the cooperation of all the population-based cancer registries in providing cancer statistics, data collection, sorting, verification and database creation. The authors assume full responsibility for analyses and interpretation of these data.
Footnote
Conflicts of Interest: The authors have no conflicts of interest to declare.
References
- Lanphear BP, Buncher CR. Latent period for malignant mesothelioma of occupational origin. J Occup Med 1992;34:718–21. [PubMed]
- Carbone M, Kanodia S, Chao A, et al. Consensus Report of the 2015 Weinman International Conference on Mesothelioma. J Thorac Oncol 2016;11:1246–62. [PubMed] DOI:10.1016/j.jtho.2016.04.028
- Chen W. updated cancer burden in China. Chin J Cancer Res 2015;27:1. [PubMed] DOI:10.3978/j.issn.1000-9604.2015.02.07
- National Cancer Center. Chinese Guideline for Cancer Registration (2016). Beijing: People’s Medical Publishing House, 2016.
- Curado MP, Edwards B, Shin HR, et al. Cancer incidence in five continents. Volume IX. IARC Sci Publ 2008:1-837.
- Parkin DM, Bray F. Evaluation of data quality in the cancer registry: principles and methods Part II. Completeness. Eur J Cancer 2009;45:756–64. [PubMed] DOI:10.1016/j.ejca.2008.11.033
- Bray F, Parkin DM. Evaluation of data quality in the cancer registry: principles and methods. Part I: comparability, validity and timeliness. Eur J Cancer 2009;45:747–55. [PubMed] DOI:10.1016/j.ejca.2008.11.032
- Kim HJ, Fay MP, Feuer EJ, et al. Permutation tests for joinpoint regression with applications to cancer rates. Stat Med 2000;19:335–51. [PubMed]
- Virta RL. USGS minerals yearbook 2009: asbestos. Reston, VA: USGS, 2009.
- Bianchi C, Bianchi T. Global mesothelioma epidemic: Trend and features. Indian J Occup Environ Med 2014;18:82–8. [PubMed] DOI:10.4103/0019-5278.146897
- National Cancer Institute. SEER Cancer Statistics Review 1975-2014. Mesothelioma-Cancer Statistics Review. Available online: https://seer.cancer.gov/csr/1975_2014/esults_merged/sect_17_mesothelioma.pdf
- Mazurek JM, Syamlal G, Wood JM, et al. Malignant mesothelioma mortality-United States, 1999-2015. MMWR Morb Mortal Wkly Rep 2017;66:214–8. [PubMed] DOI:10.15585/mmwr.mm6608a3
- Health and Safety Executive. Mesothelioma in Great Britain 2013. Mesothelioma mortality in Great Britain 1968-2011. Available online: http://www.hse.gov.uk/statistics/
- Cancer Research UK. Mesothelioma incidence statistics. Mesothelioma incidence trends over time. Available online: http://www.cancerresearchuk.org/health-professional/cancer-statistics/statistics-by-cancer-type/mesothelioma/incidence#heading-Two
- Chang KC, Leung CC, Tam CM, et al. Malignant mesothelioma in Hong Kong. Respir Med 2006;100:75–82. [PubMed] DOI:10.1016/j.rmed.2005.04.017
- Bianchi C, Bianchi T. Malignant mesothelioma in Eastern Asia. Asian Pac J Cancer Prev 2012;13:4849–53. [PubMed]
- Guo Z, Carbone M, Zhang X, et al. Improving the accuracy of mesothelioma diagnosis in China. J Thorac Oncol 2017;12:714–23. [PubMed] DOI:10.1016/j.jtho.2016.12.006
- National Institute for Occupational Safety and Health. Current intelligence bulletin 62. Asbestos fibers and other elongate mineral particles: state of the science and roadmap for research. Cincinnati, Ohio: US Department of Health and Human Services, Centers for Disease Control and Prevention, National Institute for Occupational Safety and Health, 2011. Available online: https://www.cdc.gov/niosh/docs/2011-159/pdfs/2011-159.pdf
- Liu B, van Gerwen M, Bonassi S, et al. Epidemiology of environmental exposure and malignant mesothelioma. J Thorac Oncol 2017;12:1031–45. [PubMed] DOI:10.1016/j.jtho.2017.04.002
- Bang KM, Mazurek JM, Wood JM, et al. Diseases attributable to asbestos exposure: years of potential life lost, United States, 1999-2010. Am J Ind Med 2014;57:38–48. [PubMed] DOI:10.1002/ajim.22261