
Significance of combined detection of LunX mRNA and tumor markers in diagnosis of lung carcinoma
Introduction
Detection of tumor marker (TM) has been known as a non-invasive diagnostic method and serum TMs tend to increase in early stages of tumorigenesis without positive radiological results. Currently, serum TMs commonly used in the early diagnosis of lung carcinoma include carcinoembryonic antigen (CEA), neuron-specific enolase (NSE), squamous cell carcinoma (SCC) antigen, and lung-specific X protein (LunX) (1). In recent years, as demonstrated by the concept of micro-metastasis and the progress of relevant studies, small foci of cancer cells might exist in blood circulation, bone marrow, and lymph nodes in early stages of tumorigenesis, which are undetectable by conventional methods, suggesting the possibility of distant metastases and poor prognosis (2). Therefore, early diagnosis of lung carcinoma, as well as its metastatic potential, is extraordinary important. In this study, quantitative RT-PCR and chemiluminescence immunoassay were employed to examine the peripheral profile of LunX mRNA both in patients with lung carcinoma and healthy subjects. The value of commonly used serum TMs in combination with LunX gene test in early diagnosis of lung carcinoma was evaluated.
Materials and methods
Clinical data
The peripheral blood specimens out of 113 patients with lung carcinoma admitted to Sun Yat-sen University Cancer Center from May-01-2009 to May-01-2010 (case group) were collected. All patients did not undergo any auxiliary interventions before sample collections. There were 65 males and 48 females with the age ranging from 31 to 72 years. The average age was 50 years, with the median age of 46 years. There were 52 cases of SCC, 46 cases of adenocarcinoma, and 15 cases of small cell carcinoma. According to 2012 UICC Staging System, there were 24 patients in Stage I, 30 patients in Stage II, 40 patients in Stage III, and 19 patients in Stage IV. Thirty healthy subjects were included as the control group, including 22 males and 8 females, ranging from 35 to 62 years, with a median age of 47 years.
Experimental methods
Reagents and instruments
The Reagents and Instruments used in this study included: lymphocyte separation medium (Tianjin Hao Yang Biological Products Technology Co., Ltd., China); Trizol lysis buffer (Invitrogen); DNA purification kit and plasmid extraction kit, reverse transcription reagents and real-time quantitative PCR reagents (Takara Bio); TaqMan-MGB probe (Shanghai GeneCore Biotechnology Co., Ltd., China); The primer sequences were: P1: 5'-TCATTGTCTTCTACGGGCTGTT-3'; P2: 5'-CTTGGAGCTTATGCCGAGAG-3'; TaqMan—MGB probe: 5'-CAGACCATGGC CCAGTTTGGAGGCCTG-3'. β-Actin with a length of amplified fragments of 142 bp served as the internal reference. Other instrument included ROCHE Lightcycler quantitative PCR instrument and ROCHE Mode E170 electrochemiluminescence immunoassay analyzer and diagnostic kits.
Total RNA extraction and reverse transcription
A total of 5 mL venous blood was collected from intervention-naive patients and healthy subjects. After sodium citrate treatment, nucleated cells were separated by using lymphocyte separation medium. Wash with PBS before centrifugation (6,000 r/min for 10 min under ambient conditions, with the centrifugal radius of 8.5 cm). The supernatant was transferred to a sterile 1.5 mL Ep vial and digested in Trizol 1,000 µL before chloroform extraction. The total RNA was precipitated by isopropanol and washed with 75% ethanol for two times. After air-drying procedure, 15 µL of sterile DEPC water was added to dissolve the RNA residue, followed by reverse transcription reaction or cryopreservation under –70 °C condition. Reverse transcription reaction was implemented as instructed by Invitrogen Kit instructions.
Quantitative PCR reactions
Real-time PCR amplification was optimized. 2 µL of above reverse transcription product was mixed with LunX gene fluorescent probes, P1 and P2 primers (with 1 µL for each primer) (5 µmol/L), Ex-Taq HS polymerase 1 U and 10× PCR reaction buffer (dNTP) 2.5 µL to reach 25 µL in volume. PCR conditions: 37 °C for 10 min, 95 °C for 10 min (95 °C, 15 S; 56 °C, 1 min) ×40 cycles.
Construction and identification of standard system for real-time quantitative detection of LunX gene
Reverse transcription reaction was implemented according to conventional practice with oligo dT as the primer. During the reaction, 2 µL of above reverse transcription product was mixed with P1 and P2 primers (with 1 µL for each primer) (5 µmol/L), Ex-Taq HS polymerase 1 U and 10× PCR reaction buffer (containing dNTP) 5.0 µL to reach 50 µL in volume. PCR conditions: denaturation at 94 °C for 5 min; hot initiation at 80 °C for 2 min, 94 °C 45 s, 58 °C for 30 s, 72 °C for 30 s, 30 cycles; and final extension at 72 °C for 5 min. After T-A cloning procedure and sequencing correctly identified for the purified LunX PCR product LunX gene, purified recombinant plasmid was extracted from preparations of target cloning bacteria by using plasmid extraction kit (follow the procedures as instructed). The concentration and purity were determined by UV spectrometer and were used to estimate the content of plasmid copies. Reference LunX gene with known copy numbers was diluted according to the gradient of 103-108 copies/mL to establish the standard curve after quantitative PCR amplification. The standard curve of β-actin standard was also established with the same dilution method. The expression profiles of LunX and β-actin in each specimen were estimated according to the standard curves. The number of LunX mRNA copies could be standardized through dividing the number of LunX copies by the number of β-actin copies for each sample.
Examination of three TMs
Serum profiles of CEA, NSE and CYFRA21-1 were determined as instructed by using Mode E170 electrochemiluminescence immunoassay analyzer and relevant diagnostic kits. Positive results were defined as NSE >15.2 ng/mL, CYFRA21-1 >3.3 ng/mL, and CEA >5 ng/mL.
Statistical analysis
Statistical analyses were implemented by using SPSS 13.0 statistical software. Sample frequency was analyzed by commonly used χ2 test. Categorical variables were compared by Kruskal-wallis Test, with the test level α=0.05. The sensitivity, specificity and accuracy were estimated according to the following formula described in literature (1). Sensitivity =A/(A+C)×100%; specificity =D/(B+D)×100%; accuracy = A+D/(A+B+C+D)×100% (A, number of true positive samples; B, number of false positive samples; C, number of false negative samples; D, number of true negative samples.
Results
Inter-group comparison of positive rates in peripheral blood levels of LunX mRNA, CEA, NSE and CYFRA21-1
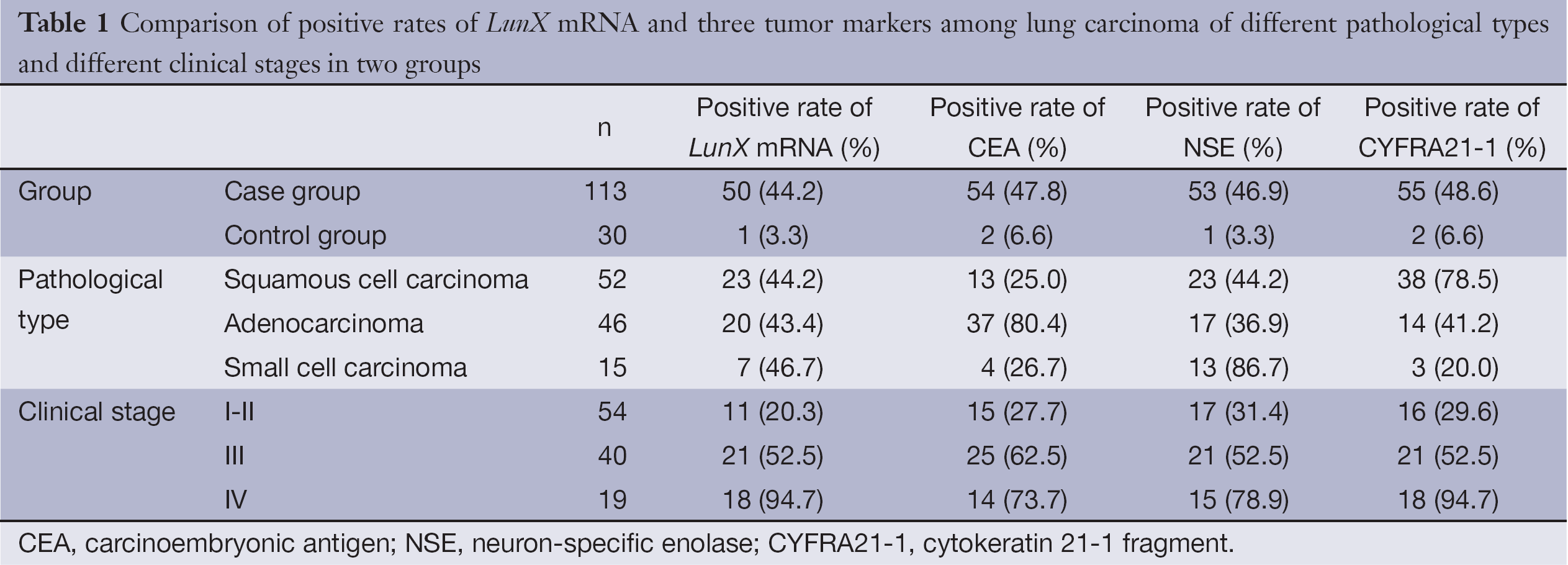
Positive results was defined as peripheral blood level of LunX mRNA >103 copies/mL. The positive rates of peripheral blood levels of LunX mRNA, CEA, NSE and CYFRA21-1 were statistically higher in NSCLC patients compared with those in controls (χ2=17.295, 16.825, 19.148, and 17.450, respectively, P<0.05) (Table 1).
Full table
Comparison of positive rates of LunX mRNA and three TMsamong lung carcinoma of different pathological types
There was no statistical significance when positive rate of LunX mRNA was evaluated among different pathological types (χ2=0.047, P>0.05). The highest CEA-positive rate was observed in the peripheral blood of patients with lung adenocarcinoma (χ2=33.154, P<0.05). The NSE-positive rate of NSCLC was significantly higher than other subtypes of lung carcinoma (χ2=11.50, P<0.05). Meanwhile, the CYFRA21-1-positive rate in SCC was significantly higher than other subtypes of lung carcinoma (χ2=23.457, P<0.05) (Table 1).
Comparison of positive rates of LunX mRNA and three TMs among lung carcinoma of TNM staging
The positive rates of peripheral LunX mRNA in patients with lung carcinoma in Stage-III and -IV were statistically significantly higher than those in Stage-I and -II (χ2=10.565, 32.462, respectively; all P<0.05). Moreover, the positive rates of peripheral CEA, NSE, and CYFRA21-1 in patients with lung carcinoma in stage-III and -IV were all significantly higher than those in stage-I and -II and the differences were statistically significant (χ2=11.333, 12.370, 4.215, 12.862, 5.036, and 23.943; all P<0.05) (Table 1).
The use of LunX mRNA and multiple TMs in combination in the diagnosis of lung carcinoma
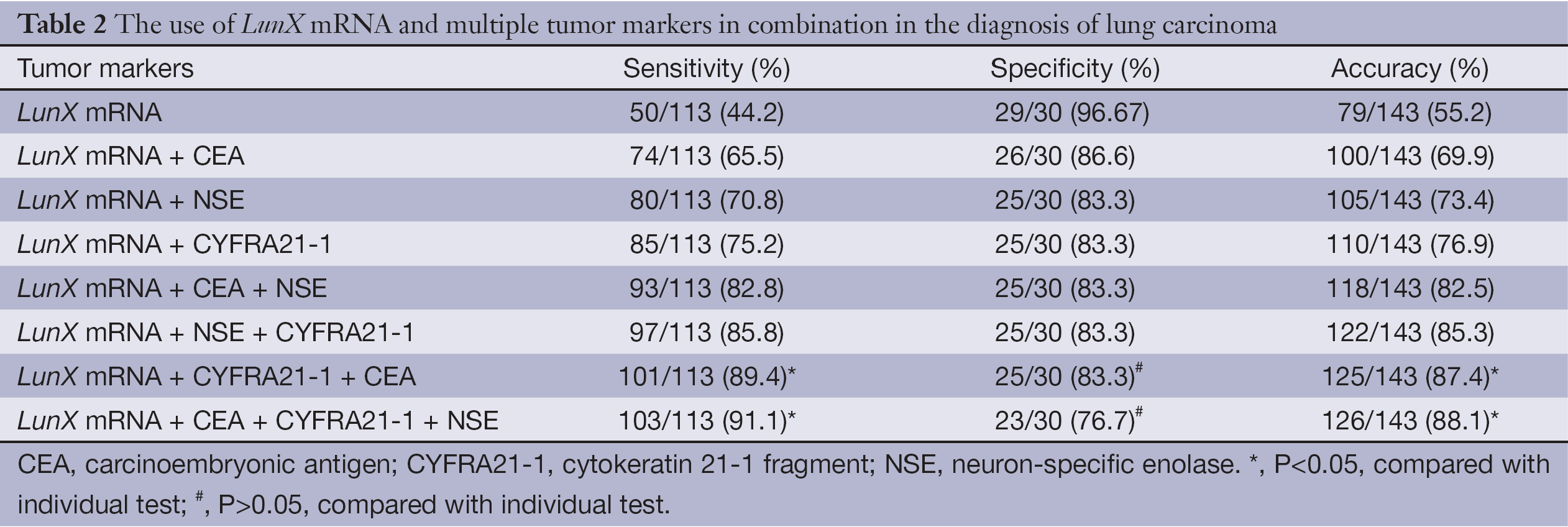
The sensitivity, specificity, and accuracy of lung carcinoma diagnosis using the individual variable of LunX mRNA were determined to be 44.2%, 96.67% and 55.2%. However, the sensitivity, specificity, and accuracy of lung carcinoma diagnosis using LunX mRNA and multiple TMs in combination were increased to 91.1%, 76.7% and 88.1%, respectively. According to the diagnostic power of this combination, the use of LunX mRNA and multiple TMs in combination could improve the sensitivity and specificity of lung carcinoma diagnosis, without significant loss of specificity (Table 2).
Full table
Discussion
TMs have been recognized to be some active substances released during the course of carcinogenesis, development, invasion and metastasis and could be observed in carcinoma and body fluid of affected patients, while they were absent or in low serum concentration non-neoplastic patients. With the progress of molecular biology and immunology, the importance of LunX, CEA, CYFRA21-1 and NSE in the diagnosis, efficacy evaluation, prediction of metastatic relapse of lung carcinoma has been concerned extensively (3).
LunX is a tissue-specific gene in human lungs by using mRNA differential display techique, as described by Iwao et al. (4) in 2001 and was demonstrated to be specifically expressed in all NSCLC tissues, as well as in healthy lung tissues. Furthermore, it is overexpressed in lung carcinoma, while its low expression or deletion was observed in other human tumor tissues (2). It is susceptible to decompose due to free mRNA is extremely susceptible to decompose due to the presence of circulating RNA cleavage enzyme. Also because of above evidence and its deletion in normal human peripheral blood cells, detection of LunX mRNA in peripheral blood theoretically suggested the presence of circulating lung cancer cells and lung cancer micro-metastases (2). In this study, the peripheral blood levels of LunX mRNA were determined to be 44.2% and 3.3% for patients with lung carcinoma and healthy subjects respectively, suggesting the LunX mRNA might be considered as a sign of lung micro-metastasis.
CEA is a class of acid glycoprotein containing a specific-determinant of human embryonic antigen and could enter into the lymphatic and blood circulation to produce elevated serum levels. It was shown to make a definite diagnosis of lung adenocarcinoma based on this TM, with the rate as high as 69.15% (3,5). In this study, the serum CEA levels were significantly higher than those of other two subtypes, suggesting its high clinical value in the diagnosis of lung adenocarcinoma, which was consistent with the literature (6-8).
Recently, CYFRA21-1 has been recommended widely as novel TMs for lung carcinoma. It is expressed in the cytoplasm of tumor cells of epithelial origin in lung carcinoma and esophageal cancer and is released into blood after cellular destruction. This TM is especially abundant in the affected tissues of lung SCC and has been recognized to be the best TM for the diagnosis of lung SCC. It has been described that the CYFRE21-1 positive rates were 50-70% (SCC), 30-50% (adenocarcinoma) and about 31 (SCLC) (sorted by decreasing order) according to the histological characteristics of lung carcinoma. The extent of increase and positive rate has been correlated to the severity of disease (5). In this study, the peripheral blood CYFRA21-1 levels in patients with lung carcinoma were significantly higher than that in patients with benign lung disease. Moreover, the expression profile of CYFRA21-1 in SCC was higher than those of adenocarcinoma and SCLC, with the positive rate of 78.5% for each individual variable, which was almost consistent with the literature (6,9).
NSE has been identified to be a TM from neuroblastoma. Since SCLC is the most frequent tumor with neuroendocrine characteristics, considerable sensitivity and specificity should be expected in case of SCLC. In this study, significant increase of peripheral blood NSE levels was observed in SCLC compared with SCC and lung adenocarcinoma, which was consistent with literature (6,10).
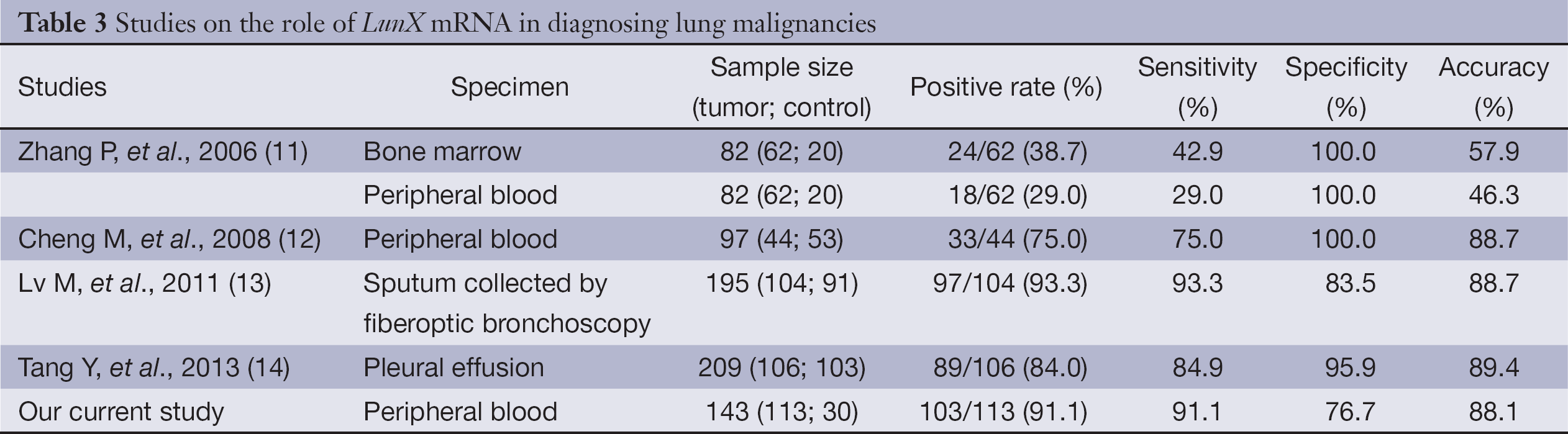
In this study, the LunX mRNA-positive rate was determined to be 44.2% for patients with non-small cell lung cancer (NSCLC), which was consistent with literature (Table 3). Moreover, the combination of LunX mRNA and TMs could improve the sensitivity and specificity of lung carcinoma diagnosis, without significant loss of specificity. The sensitivity and specificity of this diagnosis by determinations of LunX mRNA, CEA, NSE and CYFRA21-1 in combination were estimated to be 91.1% and 88.1%, respectively, which was useful for the diagnosis of lung carcinoma. The positive rates of peripheral blood concentration of LunX mRNA in patients with lung carcinoma in Stage III and IV were significantly higher than those in Stage I and II. Meanwhile, the positive rates of CEA, NSE and CYFRA21-1 tend to increase in a stage-dependent manner. These will be helpful to determine the progress and efficacy evaluation of disease, as well as the necessity to change the intervention appropriately. The positive rate of LunX mRNA was determined to be 20.3% for patients with lung carcinoma in Stage I and II. This could explain why some patients might experience recurrence and metastasis in the short term in absence of metastases as shown by CT, MRI and other radiographic examinations in early stages of disease or following radical surgery, suggesting the presence of cancer cell in the peripheral blood, resulting in formation of micro-metastasis. All these evidences showed the classical TNM staging might be supplemented by peripheral blood LunX mRNA test in order to guide treatment more accurately.
Full table
In conclusion, comprehensive investigation of the expression profiles and radiographic examinations of peripheral blood TMs might be helpful to determine the staging of lung carcinoma and to develop a reasonable comprehensive regimen. Due to the low positive rates of peripheral blood CEA, NSE and CYFRA21-1 in patients with lung carcinoma in Stage I or II, these TMs should not be used as the indicators for early tumor diagnosis. The positive rates of CEA, NSE and CYFRA21-1 were statistically different among adenocarcinoma, small cell carcinoma and SCC, suggesting somewhat importance of these TMs in the diagnosis of different pathological subtypes of lung adenocarcinoma. The use of LunX mRNA and TMs in combination could improve the sensitivity and specificity of lung carcinoma diagnosis.
Acknowledgements
This study was supported by the Guangdong Medical Science and Technology Research Fund (A2009217), the Fundamental Research Funds for the Central Universities and the grant from Youth Training Plan of Sun Yat-Sen University (No. 10ykpy38), the Research Award Fund for Outstanding Young Researchers in Sun Yat-Sen Can-cer Center (Nos. 3030451720 06 and 3030 45172005) and the Science & Technology Pillar Program of Guangdong Province (No. 2011B031800220, 2012B031800371). The authors declare their independence of sponsors, and the content of this article has not been influenced by the sponsors.
Disclosure: The authors declare no conflict of interest.
References
- Cheng M, Chen Y, Yu X, et al. Diagnostic utility of LunX mRNA in peripheral blood and pleural fluid in patients with primary non-small cell lung cancer. BMC Cancer 2008;8:156. [PubMed]
- Hermanek P, Hutter RV, Sobin LH, et al. International Union Against Cancer. Classification of isolated tumor cells and micrometastasis. Cancer 1999;86:2668-73. [PubMed]
- Ocak S, Chaurand P, Massion PP. Mass spectrometry-based proteomic profiling of lung cancer. Proc Am Thorac Soc 2009;6:159-70. [PubMed]
- Iwao K, Watanabe T, Fujiwara Y, et al. Isolation of a novel human lung-specific gene, LUNX, a potential molecular marker for detection of micrometastasis in non-small-cell lung cancer. Int J Cancer 2001;91:433-7. [PubMed]
- Benedíková A, Srovnal J, Szkorupa M, et al. Biomarkers in the detection of minimal systemic dissemination in lung cancer patients. Rozhl Chir 2012;91:209-15. [PubMed]
- Mitsuhashi N, Takahashi T, Sakurai H, et al. Establishment and characterization of a new human lung poorly differentiated adenocarcinoma cell line, GLL-1, producing carcinoembryonic antigen (CEA) and CA19-9. Lung Cancer 1995;12:13-24. [PubMed]
- Molina R, Filella X, Augé JM, et al. Tumor markers (CEA, CA 125, CYFRA 21-1, SCC and NSE) in patients with non-small cell lung cancer as an aid in histological diagnosis and prognosis. Comparison with the main clinical and pathological prognostic factors. Tumour Biol 2003;24:209-18. [PubMed]
- Tomita M, Shimizu T, Ayabe T, et al. Maximum SUV on positron emission tomography and serum CEA level as prognostic factors after curative resection for non-small cell lung cancer. Asia Pac J Clin Oncol 2012;8:244-7. [PubMed]
- Dohmoto K, Hojo S, Fujita J, et al. Mechanisms of the release of CYFRA21-1 in human lung cancer cell lines. Lung Cancer 2000;30:55-63. [PubMed]
- Ono A, Naito T, Ito I, et al. Correlations between serial pro-gastrin-releasing peptide and neuron-specific enolase levels, and the radiological response to treatment and survival of patients with small-cell lung cancer. Lung Cancer 2012;76:439-44. [PubMed]
- Zhang P, Liu Y, Chen J, et al. Feasibility and its clinical significance of detection of LUNX mRNA expression in diagnosis of micrometastasis for non-small cell lung cancer. Zhongguo Fei Ai Za Zhi 2006;9:506-10. [PubMed]
- Cheng M, Chen Y, Yu X, et al. Diagnostic utility of LunX mRNA in peripheral blood and pleural fluid in patients with primary non-small cell lung cancer. BMC Cancer 2008;8:156. [PubMed]
- Lv M, Wu MZ, Zhao YJ, et al. Expression and clinical significance of lung-specific X protein mRNA in bronchial brushing specimens from patients with or without lung cancer. Respirology 2011;16:1076-80. [PubMed]
- Tang Y, Xu L. Superiority and clinical significance of LunX mRNA in the diagnosis of malignant pleural effusion caused by pulmonary carcinoma. J Exp Clin Cancer Res 2013;32:37. [PubMed]