
Incidence, mortality and survival of female breast cancer during 2003-2011 in Jiangsu province, China
*These authors contributed equally as first authors to this study.
Abstract
Objective: To assess the incidence, mortality and survival status of female breast cancer in Jiangsu province of China.
Methods: Population-based cancer registry data in Jiangsu province were collected during 2003-2011. Crude rates, age-specific rates, age-standardized rates and annual percent changes of incidence and mortality were calculated to describe the epidemiologic characteristics and time trends. Patients diagnosed from 2003 to 2005 were chosen for analyzing the survival status of breast cancer.
Results: From 2003 to 2011, 17,605 females were diagnosed with breast cancer and 4,883 died in selected registry areas in Jiangsu province. The crude incidence rate was 25.18/100,000, and the age-standardized rates by Chinese population (ASRC) and by world population (ASRW) were 19.03/100,000 and 17.92/100,000, respectively. During the same period, the crude mortality rate was 6.98/100,000 and the ASRC and ASRW were 4.93/100,000 and 4.80/100,000, respectively. From 2003 to 2011, the incidence and mortality increased with annual percent change of 11.37% and 5.78%, respectively. For survival analysis, 1,392 patients in 7 areas were identified in 2003-2005 and finished 5 years of follow-up. Survival rates were found to decrease with survival years, the 5-year observed survival rate was 45.9% and the relative survival rate was 52.0%. We also found that the survival rate varied across the province, which was lower in the north and higher in the south of Jiangsu province.
Conclusions: Breast cancer has become a significant public health problem in Jiangsu province and China. More resources should be invested in primary prevention, earlier diagnosis and better health services in order to increase survival rates among Chinese females.
Keywords: Breast cancer; incidence; mortality; observed survival; relative survival; Jiangsu province
Submitted Mar 06, 2016. Accepted for publication Apr 25, 2016.
doi: 10.21147/j.issn.1000-9604.2016.03.06
Introduction
Breast cancer is one of the most common malignancies and has become a serious threat to women’s health around the world. In 2012,1.67 million women were diagnosed with breast cancer worldwide, accounted for 25.2% of all cancers among women. Meanwhile, 522,000 women died of breast cancer which accounted for 14.7% of all female cancer deaths in 2012 (1). Interestingly, the risk of this disease varies significantly across the world. Comparing with Western countries, the incidence and mortality of breast cancer in China are at relatively lower levels. According to the statistics of International Agency for Research on Cancer (IARC), the age-standardized incidencerate of female breast cancer in China was 22.1/100,000 in 2012, while the age-standardized mortality was 5.4/100,000 (2). However, because of the large population size, the number of cases in China is higher than that in most countries. Chen reported that there were almost 269,000 women joined the group of breast cancer in China, and the deaths were 69,500 at the same time (3).
In the past decades, incidences of female breast cancer in most countries and regions have increased by 30%-40% (4), but this increasing trend was more obvious in China. From 1980 to 1990, the crude incidence has increased by 72% with an annual growth of 3%-4%, which was far above the world average (5, 6). On the other hand, the crude mortality of breast cancer in China also increased by approximately 100% since 1970s (5.90/100,000 in 2004-2005 vs. 2.95/100,000 in 1970s) (4). The fast increase of breast cancer risk in China is partly associated with its economy booms and rapid changing lifestyles.
Comparing with cancers of high fatality such as lung cancer and liver cancer, the prognosis of breast cancer is much better (7). Population-based cancer survival could reflect the prognosis of cancer and evaluate the progress of disease control, and is also helpful in making policies to ensure improved and equitable cancer care. Besides, cancer survival can also help establish strategies to improve cancer treatment. However, only a few cancer registries have carried out population-based survival statistics for breast cancer among the Chinese people in recent years, results showed that the survival rates have been significantly improved (8-10), but still much lower than many developed countries such as the United States, Australia and some European countries (7). Being lack of historical cancer registry data, the epidemiologic characteristics of female breast cancer in China, such as long-term change of incidence, mortality and survival rates, still need further investigation.
Jiangsu province is an eastern coastal province in China with a population of 79 million. Although being one of the developed areas in China, Jiangsu province is an area with high incidence and mortality of malignant tumors. According to the Second National Death Retrospective Survey in early 1990s, the mortality of cancer was 160/100,000, which is 48.15% higher than the national average (108/100,000) (11). As a big province in China, the long-term change of female breast cancer still needs further illustration, furthermore, populationbased survival analysis of this disease has not been conducted previously yet. The purposes of this study are to describe the incidence, mortality and the temporal trend of female breast cancer in Jiangsu province, and to analyze the survival status of breast cancer patients in the province.
Materials and methods
Data source
Data were collected from Jiangsu Province Cancer Registry, which is affiliated with Jiangsu Provincial Center for Disease Control and Prevention. Cancer registry in Jiangsu province was first initiated in 1970s in Qidong County and has experienced quick development since 2000 (12). Now the whole province has been covered by cancer registry system, however, only a few counties could provide population-based registry data dating back to early 2000.
There were 7 registries providing integrate data in 2003, then with the improvement of cancer registry work, the registered points were gradually increased in the following years and until 2011 there were 29 registries providing integrate data. These data were selected to analyze the incidence and mortality of female breast cancer. For survival analysis, patients who were diagnosed as breast cancer between January 1,2003 and December 31,2005 were recruited and followed up for at least 5 years. A mix of active and passive follow-up methods was used to identify the vital status of patients from the date of diagnosis. In total, 7 counties provided complete survival information and passed quality evaluation. Among the 7 counties, 1 is in the south of Jiangsu province, 3 in the middle and 3 in the north.
Information of breast cancer patients including personal information (name, age, birth date, address, etc.) and diagnostic information (onset date, diagnostic basis, date of death, ICD- 10 code, etc.) were collected using standardized cancer registry card.
Quality control
According to the data quality standards from International Agency for Research on Cancer/International Association of Cancer Registration (IARC/IACR), Software including MSFox Pro, MS-Excel and IARCcrg Tools (IARC/IACR) was used to inspect and assess the quality of data. The reliability, validity and integrity were evaluated by major indices including proportion of morphological verification (MV%), percentage of cases diagnosed with death certification only (DCO%) and mortality to incidence ratio (M/I). In this study, the MV% of female breast cancer was 84.72%, DCO% was 0.52% and M/I was 0.28, which indicated that data quality met the criteria of data quality of breast cancer (13).
Statistical analysis
Crude incidence and mortality were calculated by using the number of new cases or death cases divided by the population inregistry areas during the same period. Rates were standardized by using 2000 Chinese standard population (ASRC) and Segi’s world population (ASRW) (14). Age-specific rates were calculated for 19 age groups. Time trends during 2003- 2011 were estimated by annual percent change (APC), which was calculated with the following formula: APC=100×(eβ-1), coordinated with the model y=α+βx+ε, wherein α is constant term, β is the slope calculated from a linear regression of log rates in a calendar year and ε means random error (15, 16).
Life-table method was utilized to compute the observed survival (OS) and Ederer Ⅱ method was used to estimate expected survival via the Stata software 12.0 (Stata Corp LP, College Station, Texas, USA) (17). In addition to OS, relative survival (RS), a comprehensive index which can represent the excess mortality of cancer when other mortality risk was removed, was also calculated by dividing the OS of patients by the expected survival of a comparable group in the general population (18). Standardized RS was adjusted by the International Cancer Survival Standards (ICSS) (19).
Results
Incidence and mortality
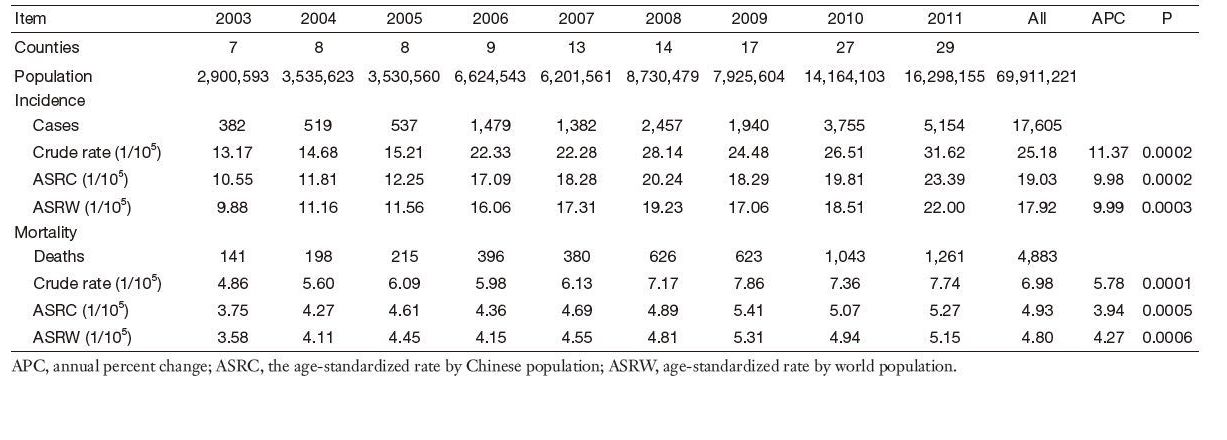
In selected cancer registry areas of Jiangsu province, from 2003 to 2011, the observed total population size was 140,465,998 and 69,911,221 were females. Meanwhile, 17,605 women were diagnosed with breast cancer, accounted for 11.72% and ranked the 4th of all female cancer cases. The annual average crude incidence was 25.18/100,000 with an ASRC and ASRW of 19.03/100,000 and 17.92/100,000, respectively. There were 4,883 women died from breast cancer during the same period, accounted for 5.09% and ranked the 6th of total female cancer deaths. The annual average crude mortality was 6.98/100,000 with the ASRC and ASRW of 4.93/100,000 and 4.80/100,000, respectively (Table 1).
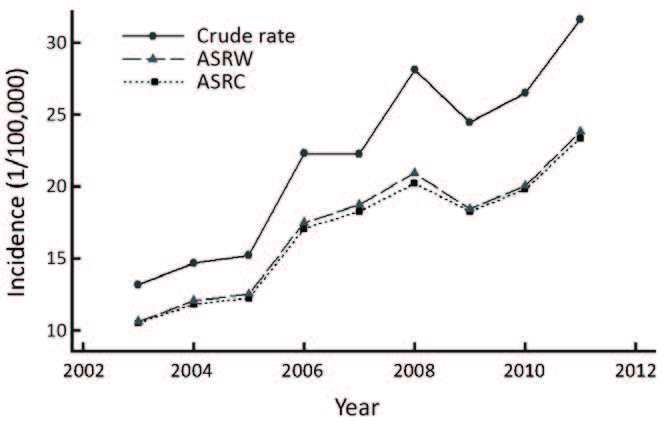
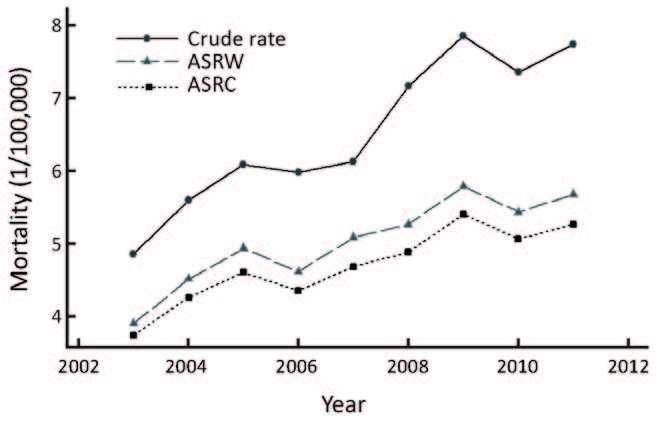
The temporal trends of breast cancer are shown in Figure 1 and Figure 2. Significant upward trends were observed for both incidence and mortality from 2003 to 2011, although there are some fluctuations between years. As listed in Table 1, the crude incidence increased from 13.17/100,000 to 31.62/100,000 with an APC of 11.37% (P < 0.01), and the crude mortality increased from 4.86/100,000 to 7.74/100,000 with an APC of 5.78% (P < 0.01). After age standardization, the increasing trends became smooth but still obvious (Figure 1, 2).
Full table
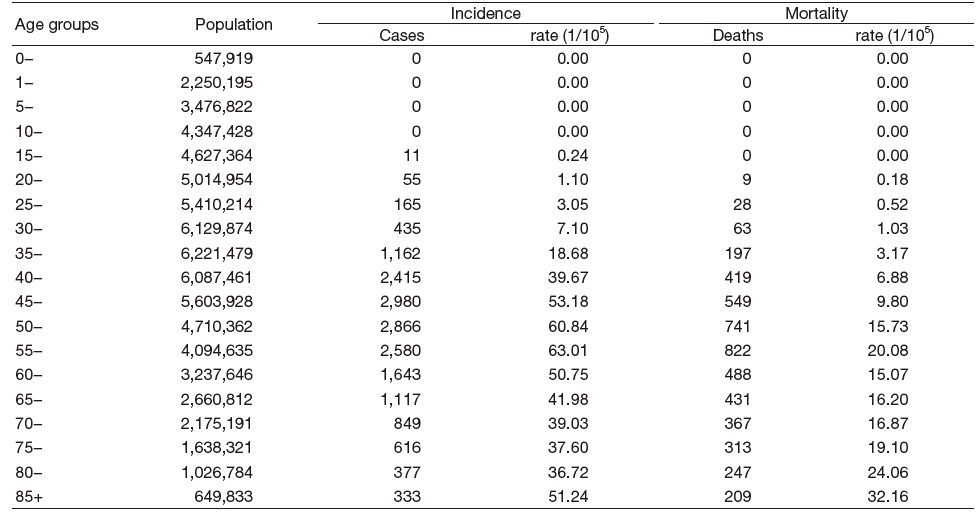
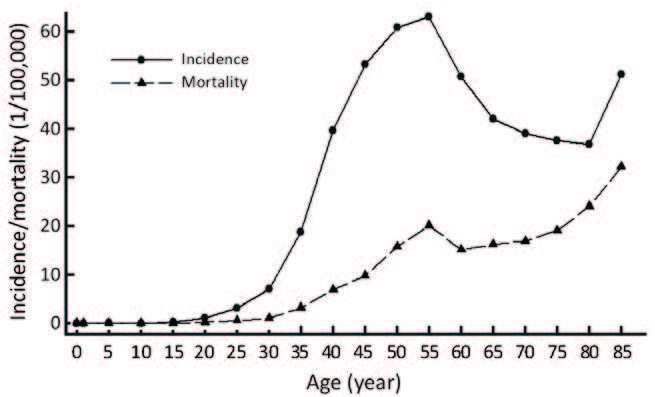
Table 2 displays the age-specific incidence and mortality of female breast cancer in registry areas of Jiangsu province. It was obvious that both incidence and motility increased with age. Among women after 30 years old, the incidence increasedrapidly with age growth and reached the peak at age of 55-59 years (63.01/100,000), then stayed at a high level and decreased slightly until 85+ years again (51.24/100,000). Similarly, the mortality also reached its first peak at age of 55-59 years (20.08/100,000), and the highest rate occurred at age of 85+ years (32.16/100,000) (Figure 3).
Full table
Survival analysis
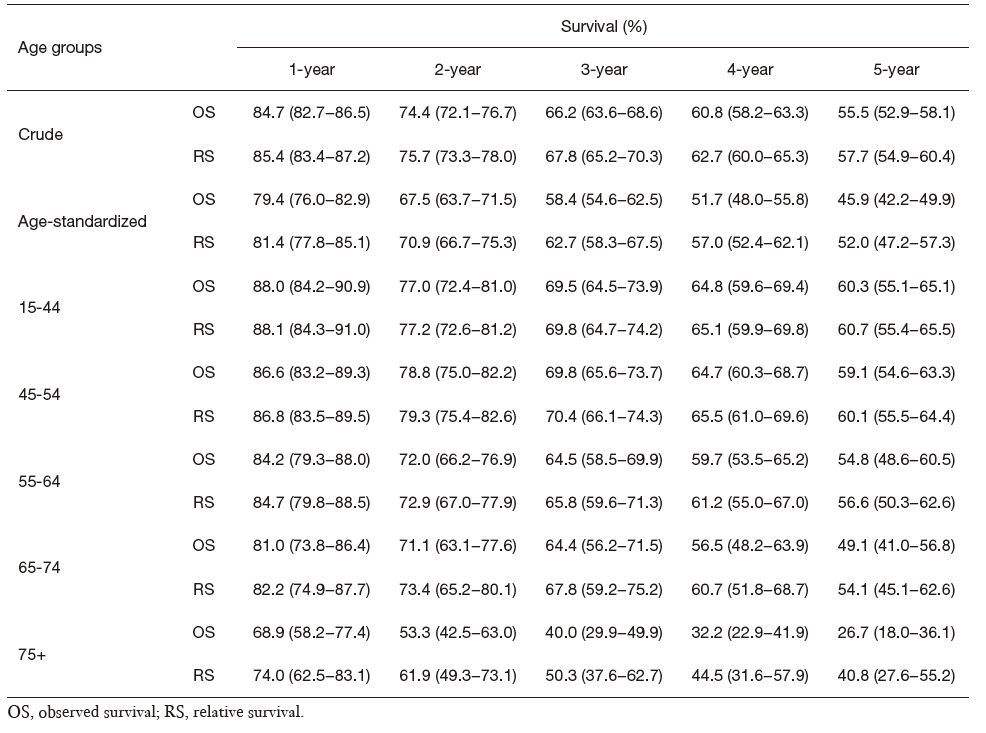
From January 1,2003 to December 31,2005, there being 1,392 breast cancer cases recruited for survival analysis in selected registry areas. All subjects were followed for at least 5 years andthe rate of loss to follow-up was 2.5%. The OS and RS from 2003 to 2005 are displayed in Table 3. The age-standardized 1-,3- and 5-year OS was 79.4% [95% confidence interval (95% CI): 76.0-82.9],58.4% (95% CI: 54.6-62.5) and 45.9% (95% CI: 42.2-49.9), respectively, while RS was 81.4% (95% CI: 77.8-85.1),62.7% (95% CI: 58.3-67.5) and 52.0% (95% CI: 47.2-57.3), respectively. Both OS and RS were found to be dropped with survival years.
Full table
The OS and RS of different ages are also shown in Table 3. For each survival year, both OS and RS declined with age. For instance, the 5-year OS of patients at age of 15-44 years was 60.3%, however, the OS dropped to 26.7% for those at age of 75+ years. The RS showed the same pattern, decreased from 60.7% to 40.8%.
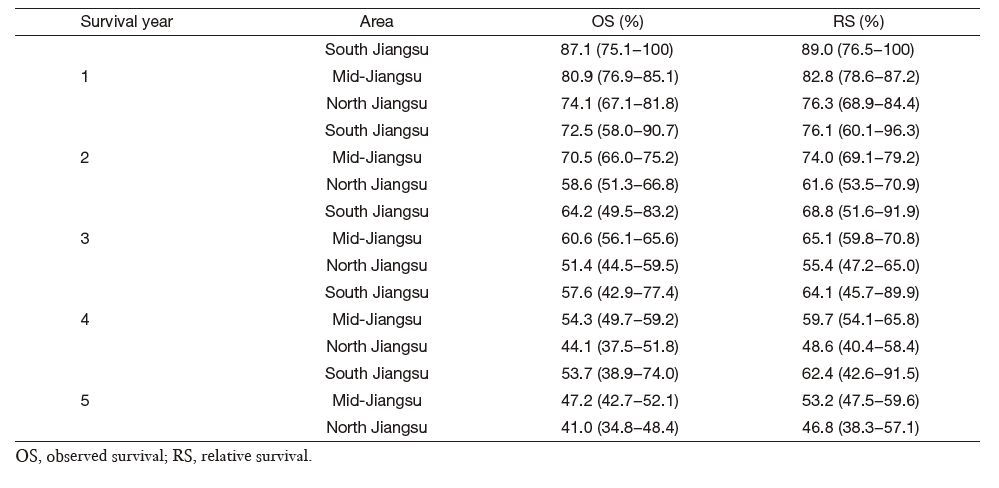
The OS and RS in different areas in Jiangsu province areshown in Table 4. The lowest survival rates were found in Northern Jiangsu province, where the 5-year OS was 41.0% and RS was 46.8%. On the contrary, the highest survival rates were observed in southern Jiangsu province where the 5-year OS was 53.7% and RS was 62.4%.
Full table
Discussion
The incidence and mortality of female breast cancer vary significantly around the world, for instance, in Northern America, the incidence is as high as 76.7/100,000, however, it is only 19.3/100,000 in Eastern Africa (20). The causes to the disparities mentioned above are complex, which have been indicated by previous researches including society, lifestyle, ethnicity, heredity, culture, environment and so on (21-23).
The incidence of breast cancer in Jiangsu province from 2003 to 2011 (ASRC=19.03/100,000) was found slightly lower than the Chinese national average (ASRC=23.27/100,000), and mortality (ASRC=4.93/100,000) was similar with the national level (ASRC=4.93/100,000) (24). Compared to other countries, the incidence of breast cancer in Jiangsu province was slightly above less developed regions, such as Tanzania, Mongolia (25) and Gambia (26), whereas it was below the world average and developed regions, such as America (20), France (27), Japan (28) and Singapore (29). Similarly, the mortality in Jiangsu province was also lower than the international average and some developed regions (2).
Although the incidence and mortality of breast cancer were relatively low in Jiangsu province compared with some regions in the world, they have increased rapidly in recent years. From 2003 to 2011, the age-standardized incidence increased from 10.55/100,000 to 23.39/100,000 and the mortality increased from 3.75/100,000 to 5.27/100,000, which shared the same tendency of China where the age-standardized incidence increased from 22.18/100,000 to 25.89/100,000 and the mortality increased from 4.80/100,000 to 6.56/100,000 during 2004 to 2010 (13,30-32). China has been experiencing the transition in both economy and lifestyle, the development of economy, the acceleration of life pace, the westernization of lifestyle, the decline of fertility and breast feeding among women, the changing of traditional diet structure and significantly increased prevalence in obesity, all of these have jointly contributed to the sharp increase of breast cancer risk in Jiangsu province as well as the whole China (33-35,22).
Historical data about survival of female breast cancer in China were insufficient. According to limited published results, the total 5-year RS in China in 2003-2005 was estimated to be 73.0%,77.8% in urban and 55.9% in rural areas (7). The 5-year RS in Jiangsu province was 52.0%, which was similar to the average level in rural areas of China, which could be explained by the fact that most areas selected for survival analysis were rural in the present research. The survival rate of breast cancer varies around the world. In comparison with other countries or regions, the 5-year RS of female breast cancer in Jiangsu province was lower than that of developed regions, such as Germany (36, 37), France (38), Korea (39), United States (40), Japan (41), Canada (42, 43), but was higher than less developed regions such as Philippines (44), Mumbai, India (43), Gambia (44), Kampala and Uganda (45). Even in China, regional disparities do exist (7). Xiang reported that the 1-,3- and 5-year RS in Shanghai from 1988 to 1991 was 89.7%,77.2% and 71.7% (10), respectively. The 5-year RS in Beijing was reported as 66.3% and 74.2% during 1982-1983 and 1987- 1988, respectively (9). In Qidong, 1-,3- and 5-year RS was 84.8%,70.4% and 63.1% from 1972 to 2011, respectively (12). The factors contributed to such variances between regions and countries are multiple, and some studies indicated that socio-economic inequalities, type of health insurance and race may affect cancer survival rate. The survival rates of patients in prosperous regions were higher than those in poverty-stricken regions. Moreover, patients who have private insurance had higher survival than other patients (46-48). Besides, variations in the prevalence of associated risk factors, public awareness of health knowledge, environmental pollution, and differences in initial treatment, supervision and support networks may be other reasons of the geographic changes (7). In this study, the difference among survival in south, middle and north Jiangsu province also supported that economic, social determinants and lifestyle may be significant influencing factors of survival rates (49, 50).
In this study, the highest 5-year RS was observed among the group of age 15-44 years and the lowest 5-year RS was observed at age of 75+ years. Elderly patients are usually in poor physical condition and may also suffer from other diseases, and thus are prone to receive more conservative treatments (40). Besides, people in this age may also lack of exercise, and previous research had shown that more physical activity did contribute to the decline of breast cancer-specific mortality as well as all-cause mortality (51). These reasons might explain why the survival rate of female breast cancer declines with age.
Early detection of breast cancer is of utmost importance to increase survival rate and reduce mortality rate. Hayat et al. (52) found that 5-year RS detected at early stage (stage Ⅰ) was much higher than those detected at late stage (stage Ⅳ). But it is unfortunate that China has no nationwide screening program for breast cancer and earlier-stage detection (53). Therefore, more resources should be allocated to primary prevention and earlier diagnosis, such as screening practices, particularly mammography screening which is more widely used in Western countries. Moreover, public awareness of the benefits of mammography and clinical breast examination in earlier-stage detection should be improved. In addition, more accessible health services should be provided for Chinese women in order to increase the enthusiasm of screening.
Limitations also existed in this study. Firstly, most cancer registries in Jiangsu province were rural areas before 2006, therefore the differences in incidence, mortality and cancer survival between rural and urban areas could not be compared. Secondly, because lacking of historical data, the long-term variations of survival rates in Jiangsu province could not be analyzed yet. Lastly, detailed information of cancer cases, such as cancer stage and histological type, were incomplete in most registries, and thus we were not able to further analyze the association between survival rates and disease (54).
Conclusions
Breast cancer has increased rapidly among Chinese women but the survival is still relatively low especially among rural areas in China. In order to reduce the burden of this disease, more resources should be allocated to primary prevention and earlier diagnosis, and more accessible health services should be provided in order to increase the positivity of screening among Chinese women.
Acknowledgements
Funding: This study was supported by World Cancer Research Found (No. WCRF 2011/RFA/473), the Fundamental Research Funds for the Central Universities, the Scientific Research Innovation Project for the Colleges and Universities Graduate Students in Jiangsu province (No. SJLX_0112), and the Project of Jiangsu Preventive Medicine (No. Y2015058).
Footnote
Conflicts of Interest: The authors have no conflicts of interest to declare.
References
- Ferlay J, Soerjomataram I, Dikshit R, et al. Cancer incidence and mortality worldwide: sources, methods and major patterns in GLOBOCAN 2012. Int J Cancer, 2015;136 :E359–E386. [PubMed]
- Ferlay J, Soerjomataram I, Ervik M, et al. GLOBOCAN 2012 v1.0, Cancer Incidence And Mortality Worldwide: IARC Cancer Base No. 11. Lyon: IARC, 2013 .
- Chen WQ, Zheng RS, Baade PD, et al. Cancer statistics in China, 2015. CA Cancer J Clin, 2016;66 :115–132. [PubMed]
- Zheng Y, Wu CX, Zhang ML. The epidemic and characteristics of female breast cancer in China. Zhongguo Ai Zheng Za Zhi (in Chinese), 2013;23 :561–569.
- Zhang ZQ, Li GC, Ye Z. The current epidemic trend of breast cancer. Zhongguo Zhong Liu (in Chinese), 2000;9 :454–455.
- Fang QY, Wu Q, Zhang XL, et al. Analysis of the prevalence of the breast cancer. Zhongguo She Hui Yi Xue Za Zhi (in Chinese), 2012;29 :333–335.
- Zeng HM, Zheng RS, Guo YM, et al. Cancer survival in China, 2003-2005: a population-based study. Int J Cancer, 2015;136 :1921–1930. [PubMed]
- Chen YS, Zhu J, Zhang YH, et al. Analysis on the survival of female breast cancer from 2001 to 2007 in Qidong city. Zhonghua Ru Xian Bing Za Zhi (Dian Zi Ban) (in Chinese), 2011;5 :8–11.
- Wang QJ, Zhu WX, Li L, et al. Cancer survival in urban Beijing. Zhongguo Zhong Liu (in Chinese), 2001;10 :17–18.
- Xiang YB, Jin F, Chen HQ, et al. Cancer survival in urban Shanghai from 1988-1991. Zhongguo Zhong Liu (in Chinese), 1996;5 :6–8.
- Wu M, Hu XS, Zhao JK, et al. The mortality of common malignancies in 1990s in Jiangsu Province. Zhongguo Zhong Liu (in Chinese), 2003;12 :378–380.
- Zhu J, Chen JG, Chen YS, et al. Female breast cancer survival in Qidong, China, 1972-2011: a population-based study. BMC Cancer, 2014;14 :318. [PubMed]
- Chen W, Zheng R, Zhang S, et al. Annual report on status of cancer in China, 2010. Chin J Cancer Res, 2014;26 :48–58. [PubMed]
- Robson B, Purdie G, Cram F, et al. Age standardisation-an indigenous standard?. Emerg Themes Epidemiol, 2007;4 :3. [PubMed]
- Xiang YB, Zhang W, Gao LF, et al. Methods for time trend analysis of cancer incidence rates. Zhonghua Liu Xing Bing Xue Za Zhi (in Chinese), 2004;25 :173–177.
- Jensen OM, Parkin DM, Mac Lennan R, et al. Cancer registration: principles and methods. Lyon: IARC, 1991 : 138 -142.
- Dickman PW, Coviello E. Estimating and modeling relative survival. Stata J, 2015;15 :186–215.
- Chia SE, Tan CS, Lim GH, et al. Incidence, mortality and survival patterns of prostate cancer among residents in Singapore from 1968 to 2002. BMC Cancer, 2008;8 :368. [PubMed]
- Corazziari I, Quinn M, Capocaccia R. Standard cancer patient population for age standardising survival ratios. Eur J Cancer, 2004;40 :2307–2316. [PubMed]
- Ferlay J, Shin HR, Bray F, et al. Estimates of worldwide burden of cancer in 2008: GLOBOCAN 2008. Int J Cancer, 2010;127 :2893–2917. [PubMed]
- Ghafoor A, Jemal A, Ward E, et al. Trends in breast cancer by race and ethnicity. CA Cancer J Clin, 2003;53 :342–355. [PubMed]
- Perry CS, Otero JC, Palmer JL, et al. Risk factors for breast cancer in East Asian women relative to women in the West. Asia Pac J Clin Oncol, 2009;5 :219–231.
- Kunst AE. Social inequalities and cancer. Ann Oncol, 2010;21 :33. [PubMed]
- Huang ZZ, Chen WQ, Wu CX, et al. Incidence and mortality of female breast cancer in China-a report from 32 Chinese cancer registries, 2003-2007. Zhong Liu (in Chinese), 2012;32: :435–439.
- Troisi R, Altantsetseg D, Davaasambuu G, et al. Breast cancer incidence in Mongolia. Cancer Causes Control, 2012;23 :1047–1053. [PubMed]
- Brinton LA, Figueroa JD, Awuah B, et al. Breast cancer in Sub-Saharan Africa: opportunities for prevention. Breast Cancer Res Treat, 2014;144 :467–478. [PubMed]
- Daubisse-Marliac L, Delafosse P, Boitard JB, et al. Breast cancer incidence and time trend in France from 1990 to 2007: a population-based study from two French cancer registries. Ann Oncol, 2011;22 :329–334. [PubMed]
- Hori M, Matsuda T, Shibata A, et al. Cancer incidence and incidence rates in Japan in 2009: a study of 32 populationbased cancer registries for the Monitoring of Cancer Incidence in Japan (MCIJ) project. Jpn J Clin Oncol, 2015;45 :884–891. [PubMed]
- Ly D, Forman D, Ferlay J, et al. An international comparison of male and female breast cancer incidence rates. Int J Cancer, 2013;132 :1918–1926. [PubMed]
- Chen WQ, Zheng RS. Incidence, mortality and survival analysis of breast cancer in China. Zhongguo Zhong Liu Lin Chuang (in Chinese), 2015;42 :668–674.
- Zhang SW, Chen WQ, Lei ZL, et al. A report of cancer incidence from 37 cancer registries in China, 2004. Zhongguo Zhong Liu (in Chinese), 2008;17 :909–912.
- Chen WQ, Zhang SW, Kong LZ, et al. Cancer mortality report of 34 cancer registries in China, 2004. Zhongguo Zhong Liu (in Chinese), 2008;17 :913–916.
- Stoll BA. Western diet, early puberty, and breast cancer risk. Breast Cancer Res Treat, 1998;49 :187–193. [PubMed]
- Robles SC, Galanis E. Breast cancer in Latin America and the Caribbean. Rev Panam Salud Publica, 2002;11 :178–185. [PubMed]
- Shi XJ, Au WW, Wu KS, et al. Mortality characteristics and prediction of female breast cancer in China from 1991 to 2011. Asian Pac J Cancer Prev, 2014;15 :2785–2791. [PubMed]
- Holleczek B, Jansen L, Brenner H. Breast cancer survival in Germany: a population-based high resolution study from Saarland. PLoS One, 2013;8 :e70680. [PubMed]
- Brenner H, Stegmaier C, Ziegler H. Long-term survival of cancer patients in Germany achieved by the beginning of the third millenium. Ann Oncol, 2005;16 :981–986. [PubMed]
- Grosclaude P, Colonna M, Hedelin G, et al. Survival of women with breast cancer in France: variation with age, stage and treatment. Breast Cancer Res Treat, 2001;70 :137–143. [PubMed]
- Jung KW, Won YJ, Kong HJ, et al. Cancer statistics in Korea: incidence, mortality, survival and prevalence in 2010. Cancer Res Treat, 2013;45 :1–14. [PubMed]
- Holleczek B, Brenner H. Trends of population-based breast cancer survival in Germany and the US: decreasingdiscrepancies, but persistent survival gap of elderly patients in Germany. BMC Cancer, 2012;12 :317. [PubMed]
- Tsukuma H, Ajiki W, Ioka A, et al. Survival of cancer patients diagnosed between 1993 and 1996: A collaborative study of population-based cancer registries in Japan. Jpn J Clin Oncol, 2006;36 :602–607. [PubMed]
- Coleman MP, Forman D, Bryant H, et al. Cancer survival in Australia, Canada, Denmark, Norway, Sweden, and the UK, 1995-2007 (the International Cancer Benchmarking Partnership): an analysis of population-based cancer registry data. Lancet, 2011;377 :127–138. [PubMed]
- Kim Y, Yoo KY, Goodman MT. Differences in incidence, mortality and survival of breast cancer by regions and countries in Asia and contributing factors. Asian Pac J Cancer Prev, 2015;16 :2857. [PubMed]
- Sankaranarayanan R, Swaminathan R, Brenner H, et al. Cancer survival in Africa, Asia, and Central America: a population-based study. Lancet Oncol, 2010;11 :165–173. [PubMed]
- Gondos A, Brenner H, Wabinga H, et al. Cancer survival in Kampala, Uganda. British J Cancer, 2005;92 :1808–1812.
- Berrino F, Gatta G, Sant M, et al. The EUROCARE study of survival of cancer patients in Europe: aims, current status, strengths and weaknesses. Eur J Cancer, 2001;37 :673–677. [PubMed]
- Coleman MP, Babb P, Sloggett A, et al. Socioeconomic inequalities in cancer survival in England and Wales. Cancer, 2001;91 :208–216. [PubMed]
- Li CI, Malone KE, Daling JR. Differences in breast cancer stage, treatment, and survival by race and ethnicity. Arch Int Med, 2003;163 :49–56. [PubMed]
- Coleman MP, Rachet B, Woods LM, et al. Trends and socioeconomic inequalities in cancer survival in England and Wales up to 2001. British J Cancer, 2004;90 :1367–1373.
- Qin Y, Hu XS, Zhao JK, et al. Regression analysis on liver cancer and geographic factors in Jiangsu Province. Zhongguo Zhong Liu (in Chinese), 2003;12 :630–632.
- Ballard-Barbash R, Friedenreich CM, Courneya KS, et al. Physical activity, biomarkers, and disease outcomes in cancer survivors: a systematic review. J Natl Cancer Inst, 2012;104 :815–840. [PubMed]
- Hayat MJ, Howlader N, Reichman ME, et al. Cancer statistics, trends, and multiple primary cancer analyses from the surveillance, epidemiology, and end results (SEER) program. Oncologist, 2007;12 :20–37. [PubMed]
- Fan L, Strasser-Weippl K, Li JJ, et al. Breast cancer in China. Lancet Oncol, 2014;15 :e279–e289. [PubMed]
- Eisemann N, Waldmann A, Katalinic A. Imputation of missing values of tumour stage in population-based cancer registration. BMC Med Res Method, 2011;11 :129.