
Simultaneous hepatic resection benefits patients with synchronous colorectal cancer liver metastases
Abstract
Objective: The safety of the simultaneous resection of synchronous colorectal cancer liver metastases (SCRLM) is still being debated. However, this simultaneous operative approach is more commonly adopted at present than in the past. Therefore, we compared simultaneous hepatic resection with delayed hepatic resection in this study.
Methods: All patients with SCRLM diagnosed before initial treatment between January 2009 and September 2013 were retrospectively included in our study. Short-term and long-term outcomes were compared in patients who underwent simultaneous colorectal and hepatic resection and those treated by delayed hepatectomy.
Results: Among the 73 patients diagnosed with SCRLM, simultaneous colorectal and hepatic resection was performed in 60 patients (82.2%), while delayed hepatic resection was performed in 13 patients (17.8%). The mortality rate was zero. The postoperative complication rate after delayed resection was higher than, but not significantly different from, that after simultaneous resection (46% vs. 23%, P=0.166). The duration of operating time (240 vs. 420 min, P<0.05) and postoperative hospital stay time (11 vs. 18 days, P<0.05) were shorter in the simultaneous resection group. After the initial treatments were given, the 1-, 2-, and 3-year survival rates in the simultaneous resection group were 77%, 59%, and 53%, respectively, whereas those in the delayed resection group were 67%, 42%, and 10%, respectively. The 5-year survival rate in the simultaneous resection group was 23%; overall survival differed significantly between the two groups (P=0.037). Median disease-free survival (DFS) times were 19.1 months in the simultaneous resection group and 8.8 months in the delayed resection group. DFS differed significantly between the two groups.
Conclusions: Simultaneous colorectal and hepatic resection is safe and exhibits advantages in the long-time survival of patients.
Keywords: Colorectal cancer; synchronous liver metastases; simultaneous resection; survival
Submitted Jul 12, 2015. Accepted for publication Jan 08, 2016.
doi: 10.21147/j.issn.1000-9604.2016.05.08
Introduction
Colorectal cancer is one of the most common malignancies worldwide (1). Nearly half of colorectal cancer patients develop colorectal liver metastases (CRLM) during the course of the disease (2). Liver metastasis is the main cause of failure of colorectal cancer treatment (3). Synchronous liver metastases, which indicate poor outcome, represent 13% to 25% of all liver metastases from colorectal cancer (4,5). Without treatment, patients have a median survival time of 2.3 to 21.3 months (6,7). Liver resection has a pivotal role in offering long-term survival to patients with CRLM. Five-year survival rates ranging from 20% to 40% have been reported (8-10). However, the optimal surgical strategy for resectable synchronous CRLM is still being debated and continues to evolve (11-13). The classical approach is to resect the primary colorectal tumor first, and then to proceed with liver resection after 2-3 months, with chemotherapy in the interim. This policy enables the selection of the best candidates for surgery (12). With improvements in surgical techniques worldwide, the safety and efficacy of the simultaneous resection of colorectal and liver tumors has been confirmed (14-16). Some studies have found the advantages of simultaneous resection of primary colorectal tumor and synchronous liver metastases to be economical (17) and psychological (18). The present study was conducted to investigate the safety and survival superiority of simultaneous hepatic resection compared with delayed hepatectomy.
Materials and Methods
Patient selection
With the approval of the Institutional Review Board, the data of 256 consecutive patients with synchronous colorectal cancer liver metastases (SCRLM) (diagnosed before primary tumor surgery) treated with surgery at the Abdominal Surgery Department, Cancer Hospital of the Chinese Academy of Medical Science, Beijing, China between January 2009 and September 2013 were retrospectively reviewed. After ruling out patients who did not undergo complete colorectal or liver operation, 73 patients (28.5%) who received curative resection were enrolled in this study. Among the enrolled patients, 60 were treated with simultaneous hepatic resection, whereas the remaining 13 were treated with delayed hepatic resection. Radio-frequency ablation (RFA) for liver tumors smaller than 3 cm was considered as an acceptable curative treatment modality if resection was technically infeasible (i.e., if the resultant liver remnant would not have sufficient volume).
Preoperative investigation
Colonoscopy and biopsy were performed in each patient to confirm the primary tumor. Diagnosis of liver metastases was performed based on the detection of liver tumors by ultrasonography and computed tomography (CT) and/or magnetic resonance imaging (MRI). Before hepatic resection, all patients underwent contrast enhanced abdominal-pelvic multislice CT and chest X-ray, thoracic CT, or positron emission tomography-CT to rule out extrahepatic diseases. Preoperative chemotherapy was administered if the metastatic tumors were considered potentially resectable. Furthermore, patients diagnosed with initially resectable liver metastases were frequently treated by neoadjuvant chemotherapy when at least two nodes were present. Response to chemotherapy was evaluated radiologically every 2 months according to the World Health Organization guidelines and the Response Evaluation Criteria in Solid Tumors (19).
Simultaneous colorectal and hepatic resection was performed on patients without general contraindications as a combined surgical strategy (such as cardiovascular or pulmonary comorbidity) when both the primary tumor and all metastatic nodes could be resected curatively. A multidisciplinary team (MDT) that consisted of surgical oncologists, medical oncologists, radiation oncologists, pathological oncologists, and radiologists made the treatment decisions for the patients.
Surgical treatment
All the patients were operated to achieve a curative treatment. Six patients were initially treated with colorectal surgery outside our hospital. Then, then we performed delayed hepatic resection on these patients after MDT discussions. Seven patients were operated twice because of the heterogeneity of primary and metastatic tumor progression or inappropriate general conditions. The operative modalities included two incisions laparotomy (65.7%), one incision laparotomy (15.1%), laparoscopic operation combined with laparotomy (13.7%), and total laparoscopic operation (5.5%). Laparoscopic operations of the colorectum and/or liver were performed on selected patients. Preoperative MRI results of the liver were scrutinized if laparoscopic hepatic resection was planned. If a simultaneous resection strategy was selected, then hepatic resection was first performed because it represented the non-contaminated part of the procedure. However, combined laparoscopic colorectal operation must first be performed because of its infeasibility after liver laparotomy. During the operation, extensive exploration and intraoperative ultrasonography of the liver were performed routinely to rule out extrahepatic diseases and detect unsuspected liver metastases. RFA was performed for metastases smaller than 3 cm. Hepatic vascular exclusion techniques were used to decrease intraoperative blood loss when necessary. Postoperative complications were graded according to the method described by Dindo et al. (20). For safety analyses, the patients were divided into two groups: (I) patients who either had no postoperative complication or had complications that did not require intervention (Clavien-Dindo Grade I) and (II) patients who required intervention (Clavien-Dindo Grade II or higher).
Follow-up and statistical analysis
Intraoperative data were collected through medical records. Pathological analyses were performed to obtain the pathological tumor node metastasis (pTNM) stage according to the Union for International Cancer Control classification, the differentiation grade of the primary tumor, the greatest diameter, as well as the number and grade of synchronous liver metastases. Patients were followed up clinically with physical examination, estimation of serum tumor markers and liver function parameters, and abdominal ultrasonography 1 month after surgery, and then every 3 months thereafter. Abdominal-pelvic CT and/or liver MRI were performed every 6 months. Adjuvant chemotherapy was recommended routinely because of the stage IV disease.
Overall survival (OS) was defined as the time from the first treatment (surgery or chemotherapy) to the date of death (all-cause mortality). Disease-free survival (DFS) was defined as the time from the hepatic surgery to the date of the first evidence of recurrence (local, regional, or metastatic). Follow-up time was defined as the time from the hepatic surgery to the date of the last follow-up. Follow-up and survival times were recorded in months.
Data were analyzed using the SPSS 20.0 software. The comparison of categorical variables was performed by a chi-squared test (χ2) test and Fisher's exact test, continuous data by the Student t-test and Mann-Whitney U test, respectively. Cumulative survival was calculated using the Kaplan-Meier method; differences were analyzed with the log-rank test. Variables with a significant difference between simultaneous resection group and delayed resection group were entered into a Cox regression analysis. A difference was considered significant at P<0.05 (two-sided).
Results
From January 2009 to September 2013, 73 primary colorectal cancer patients who presented synchronous liver metastases detected before operation were treated curatively. Simultaneous resection of liver metastases and primary colorectal cancer was performed in 60 patients (82.2%), whereas delayed hepatic resection was performed in 13 patients (17.8%). The mean age, sex ratio, comorbidity, primary site, pathological differentiation, maximum size of the liver metastases, local tumor node (TN) stage of the primary tumor, and type of hepatectomy did not differ between the two groups. Before hepatic resection, a higher proportion of patients in the delayed resection group received chemotherapy (92.3% vs. 38.3% in the simultaneous group; P<0.05). The number of metastases was significantly smaller in the simultaneous resection group (P<0.05). The bilobar distribution of metastases was considerably more common in the delayed resection group (P<0.05). And the tumors in delayed resection group had more aggressive T stage (P<0.05), as shown in Table 1.
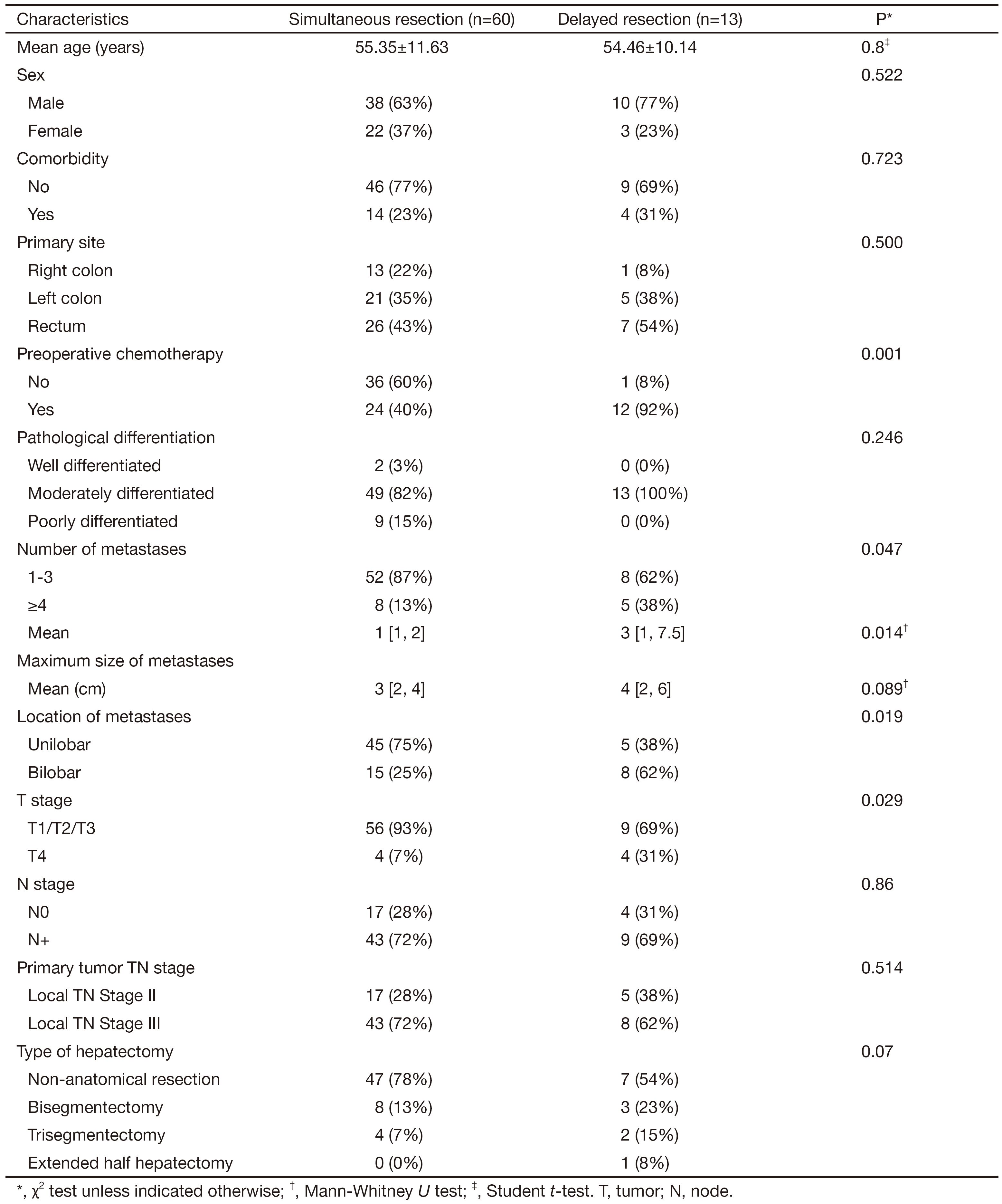
Full table
Surgical data and outcome
The type and extent of liver resections are recorded in Table 2. The intro-operative blood loss, requirements for intraoperative transfusion, hepatic pedicle occlusion, and combined RFA did not significantly differ between the two groups.
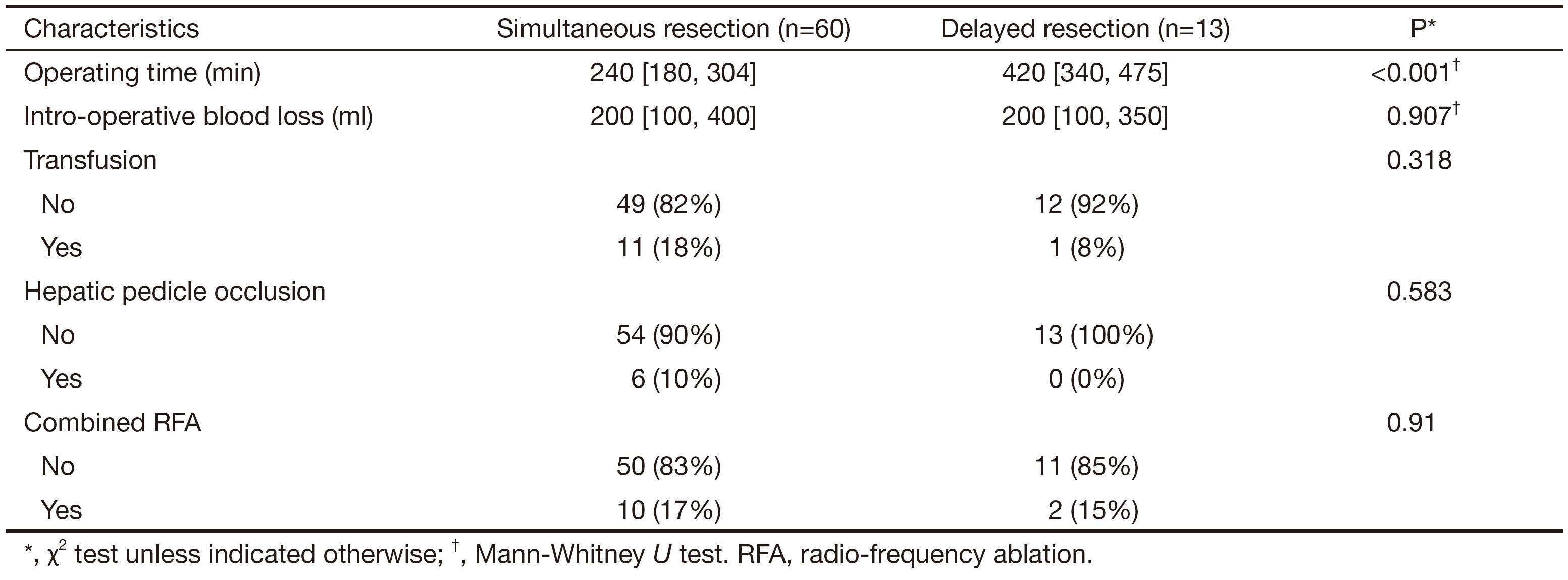
Full table
The mortality rate was zero. The postoperative complication rate (morbidity) after delayed resection was higher, but not significantly different from that after simultaneous resection (46% vs. 23%, P=0.166). The details of the postoperative complications are shown in Table 3. None of the patients required repeated operation, including the patient with abdominal hemorrhage. The duration of the operating time (240 vs. 420 min, P<0.05) and postoperative hospital stay time (11 vs. 18 days, P<0.05) were shorter in the simultaneous resection group (Tables 2 and 3).
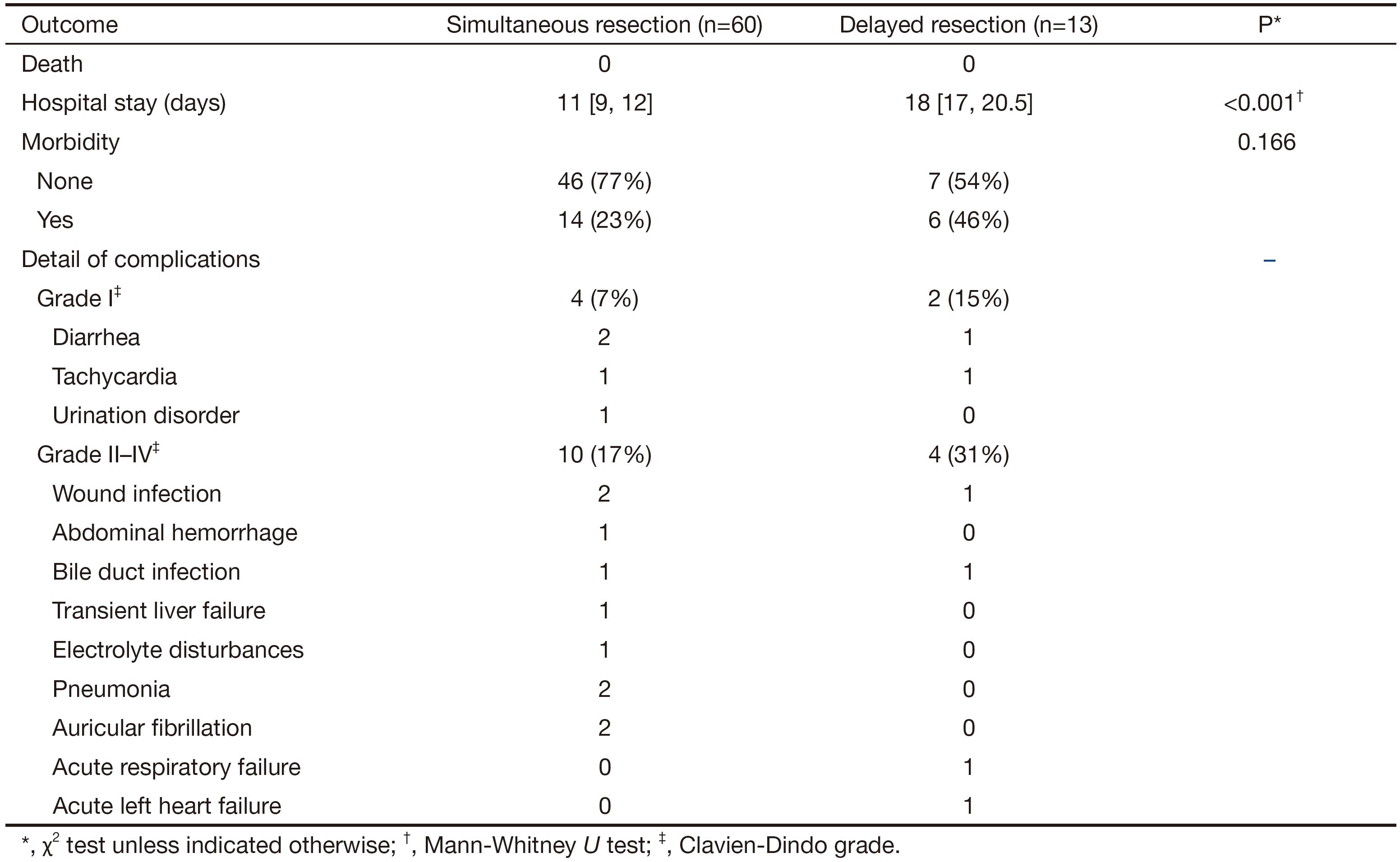
Full table
Survival and recurrence
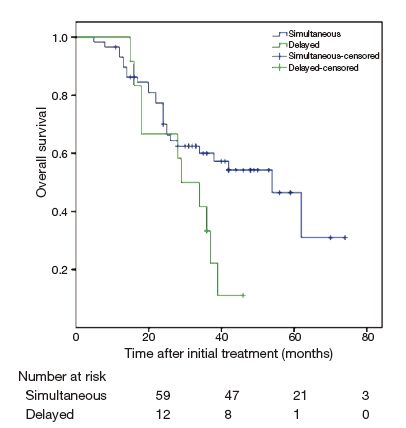
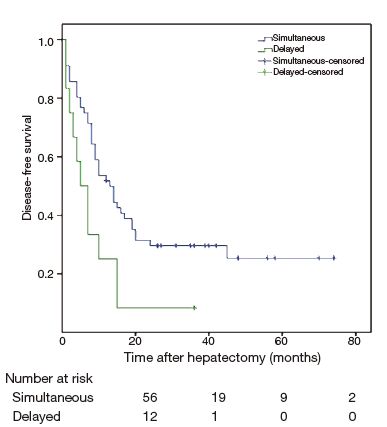
The follow-up rate of all patients was 97.4%; only two patients were lost to follow-up. The median follow-up time of all patients was 44 (range 5-74) months. After initial treatments were given, the 1-, 2-, and 3-year survival rates in the simultaneous resection group were 77%, 59%, and 53%, respectively, whereas those in the delayed resection group were 67%, 42%, and 10%, respectively (Figure 1). The 5-year survival rate in the simultaneous resection group was 23%. OS differed significantly between the two groups (P=0.037). The median DFS times were 19.1 months in the simultaneous resection group and 8.8 months in the delayed resection group. DFS differed significantly between the two groups (Figure 2, P=0.02).
Multivariate analysis was conducted to clarify the impact of the four differences (preoperative chemotherapy, number of metastases, location of metastases and T stage) between the two groups on overall survival. The results of the multivariate analysis for influence of survival are depicted in Table 4. Simultaneous resection, preoperative chemotherapy and location of metastases revealed statistically significant influence on survival.

Full table
Discussion
Although the surgical resection of both the primary tumor and liver metastases is the only option offered for a potential cure, the optimal surgical strategy for synchronous CRLM remains unclear. Our unit has adopted an active policy of simultaneously resecting CRLM irrespective of the age of the patient and metastatic tumor number, provided that complete resection of the tumors is deemed feasible, liver function reserve is satisfactory, and patient physical status is available.
In recent years, Luo et al. (21) reported that the operating time required for simultaneous and delayed resections was 255 and 415 min, intraoperative blood loss was 400 and 650 mL, and postoperative hospitalization time was 8 and 14 days, respectively. The differences were statistically significant (all P<0.0001). Our study included 60 simultaneous resection patients and 13 delayed resection patients. The results of our study were similar to those reported in previous research. In our study, the mean duration of operating time required for simultaneous and delayed resections was 240 and 420 min, while postoperative hospitalization time was 11 and 18 days, respectively (all P<0.05). However, intro-operative blood loss (200 vs. 200 mL) and transfusion rate (18% vs. 8%) were not different in the two groups (all P>0.05).
Although no perioperative death occurred in our study, the serious complication (Grade II-IV) rate was higher in the delayed resection group. This result may be attributed to the fact that the number and maximum size of the metastases are larger in the delayed resection group. Meanwhile, we observed that a higher proportion of patients in the delayed resection group received preoperative chemotherapy, which might have caused chemotherapy-associated steatohepatitis, even blue liver syndrome, and increased perioperative morbidity (22).
Unlike the results of most previous studies, which found survival benefit in the delayed resection group (23) or no survival advantage in the simultaneous group (24,25), we found that simultaneous resection had a positive influence on the OS and DFS of the patients compared with delayed resection (Figures 1 and 2).
Some authors favor delayed resection because it appears safer (16) and allows a “test of time” to detect more occult liver metastases than simultaneous resection (18). In the past decades, however, surgical techniques had stepped forward remarkably, and minimally invasive means, such as laparoscopic operation and RFA, had been widely used in surgeries, which caused less surgical trauma. Simultaneous resection had been proven to be as safe as delayed resection (24). At the same time, Gd-EOB-DTPA [Primovist(R)] enhanced MRI and intraoperative ultrasound examination improved the capability to detect micro colorectal liver metastasis lesions. The benefit of delayed resection had decreased. In addition, the waiting time before delayed hepatic resection may cause metastases to be at risk of progression. In view of tumor biology, simultaneous resection may alleviate tumor burdens without delay, achieve better chemotherapy response, and avoid repeated postoperative immunosuppression. Thus, we recommend simultaneous resection to SCRLM patients in our hospital.
This study has several limitations. The groups differ in three aspects, namely, the extent of liver resection (although insignificant), acceptance of pre-operative chemotherapy and the severity of liver metastases, which can explain the poorer OS and DFS in the delayed resection group. As was showed in multivariate analysis, simultaneous/delayed resection, preoperative chemotherapy and location of metastases were three independent prognostic factors. In spite of the liver injury, pre-operative chemotherapy provides several benefits. It can: (I) suppress tumor proliferation, improve the R0 removal rate and preserve residual liver as much as possible; (II) help physicians to evaluate the sensitivity of the chemotherapy regimen; (III) control the tiny subclinical lesions, reduce postoperative recurrence rate.
Unlike in previous studies in which surgical strategies on simultaneous and delayed hepatic resections were vacillating (16,18,21,23,25,26), we adopted an active policy of simultaneously resecting CRLM if the oncological, surgical, and general conditions of a patient permit such procedure. Despite these limitations, we can draw the conclusion that patients with SCRLM will have better chances of survival if they are qualified to undertake simultaneous hepatic resection.
Conclusions
We presented the outcomes of simultaneous and delayed liver metastases resections conducted in our hospital. Our results revealed that simultaneous resection did not increase the risk of postoperative complications and presented a positive effect on the OS and DFS of patients compared with delayed resection. Moreover, simultaneous resection had shorter operating time and postoperative hospitalization stay. These results support the conclusion that simultaneous resection of SCLRM is a safe procedure and offers advantages in the long-time survival of patients.
Acknowledgements
Funding: This study was supported by the National High-Tech R&D Program (863 Program) of China (2015AA020408), the National Natural Science Foundation of China (81201967, 31470073), the Beijing Natural Science Foundation (7132193, 7144238), the Capital Health Research and Development of Special (2014-1-4022) and Beijing Nova Program (No. 2009A69).
Footnote
Conflicts of Interest: The authors have no conflicts of interest to declare.
References
- Chen W. Cancer statistics: updated cancer burden in China. Chin J Cancer Res 2015;27:1. [PubMed]
- Adam R. Colorectal cancer with synchronous liver metastases. Br J Surg 2007;94:129–31. [PubMed] DOI:10.1002/(ISSN)1365-2168
- Amatu A, Bencardino K, Sartore-Bianchi A, et al. Aspirin for colorectal cancer with PIK3CA mutations: the rising of the oldest targeted therapy. Ann Transl Med 2013;1:12. [PubMed]
- Cady B, Monson DO, Swinton NW. Survival of patients after colonic resection for carcinoma with simultaneous liver metastases. Surg Gynecol Obstet 1970;131:697–700. [PubMed]
- Clark ME, Smith RR. Liver-directed therapies in metastatic colorectal cancer. J Gastrointest Oncol 2014;5:374–87. [PubMed]
- Luna-Perez P, Rodriguez-Coria DF, Arroyo B, et al. The natural history of liver metastases from colorectal cancer. Arch Med Res 1998;29:319–24. [PubMed]
- Stangl R, Altendorf-Hofmann A, Charnley RM, et al. Factors influencing the natural history of colorectal liver metastases. Lancet 1994;343:1405–10. [PubMed] DOI:10.1016/S0140-6736(94)92529-1
- Hughes KS, Simon R, Songhorabodi S, et al. Resection of the liver for colorectal carcinoma metastases: a multi-institutional study of patterns of recurrence. Surgery 1986;100:278–84. [PubMed]
- Jaeck D, Bachellier P, Guiguet M, et al. Long-term survival following resection of colorectal hepatic metastases. Association Fran.aise de Chirurgie. Br J Surg 1997;84:977–80. [PubMed] DOI:10.1002/(ISSN)1365-2168
- Fong Y, Blumgart LH. Hepatic colorectal metastasis: current status of surgical therapy. Oncology (Williston Park) 1998;12:1489–98. [PubMed]
- Elias D, Detroz B, Lasser P, et al. Is simultaneous hepatectomy and intestinal anastomosis safe. Am J Surg 1995;169:254–60. [PubMed] DOI:10.1016/S0002-9610(99)80146-9
- Lambert LA, Colacchio TA, Barth RJ Jr. Interval hepatic resection of colorectal metastases improves patient selection. Arch Surg 2000;135:473–9. [PubMed] DOI:10.1001/archsurg.135.4.473
- Krawczyk M. Risk of synchronous and metachronous liver resection for colorectal cancer metastases. Przegl Lek 2000;57:40–2. [PubMed]
- Martin R, Paty P, Fong Y, et al. Simultaneous liver and colorectal resections are safe for synchronous colorectal liver metastasis. J Am Coll Surg 2003;197:233–41. [PubMed] DOI:10.1016/S1072-7515(03)00390-9
- Sasanuma H, Yasuda Y, Mortensen FV, et al. Simultaneous colorectal and liver resections for synchronous colorectal metastases. Scand J Surg 2006;95:176–9. [PubMed]
- Reddy SK, Pawlik TM, Zorzi D, et al. Simultaneous resections of colorectal cancer and synchronous liver metastases: a multi-institutional analysis. Ann Surg Oncol 2007;14:3481–91. [PubMed] DOI:10.1245/s10434-007-9522-5
- Abbott DE, Cantor SB, Hu CY, et al. Optimizing clinical and economic outcomes of surgical therapy for patients with colorectal cancer and synchronous liver metastases. J Am Coll Surg 2012;215:262–70. [PubMed] DOI:10.1016/j.jamcollsurg.2012.03.021
- Weber JC, Bachellier P, Oussoultzoglou E, et al. Simultaneous resection of colorectal primary tumour and synchronous liver metastases. Br J Surg 2003;90:956–62. [PubMed] DOI:10.1002/(ISSN)1365-2168
- Therasse P, Arbuck SG, Eisenhauer EA, et al. New guidelines to evaluate the response to treatment in solid tumors. European Organization for Research and Treatment of Cancer, National Cancer Institute of the United States, National Cancer Institute of Canada. J Natl Cancer Inst 2000;92:205-16. [PubMed]
- Dindo D, Demartines N, Clavien PA. Classification of surgical complications: a new proposal with evaluation in a cohort of 6336 patients and results of a survey. Ann Surg 2004;240:205–13. [PubMed] DOI:10.1097/01.sla.0000133083.54934.ae
- Luo Y, Wang L, Chen C, et al. Simultaneous liver and colorectal resections are safe for synchronous colorectal liver metastases. J Gastrointest Surg 2010;14:1974–80. [PubMed] DOI:10.1007/s11605-010-1284-x
- Bilchik AJ, Poston G, Curley SA, et al. Neoadjuvant chemotherapy for metastatic colon cancer: a cautionary note. J Clin Oncol 2005;23:9073–8. [PubMed] DOI:10.1200/JCO.2005.03.2334
- de Haas RJ, Adam R, Wicherts DA, et al. Comparison of simultaneous or delayed liver surgery for limited synchronous colorectal metastases. Br J Surg 2010;97:1279–89. [PubMed] DOI:10.1002/bjs.7106
- Slesser AA, Simillis C, Goldin R, et al. A meta-analysis comparing simultaneous versus delayed resections in patients with synchronous colorectal liver metastases. Surg Oncol 2013;22:36–47. [PubMed] DOI:10.1016/j.suronc.2012.11.002
- Moug SJ, Smith D, Leen E, et al. Evidence for a synchronous operative approach in the treatment of colorectal cancer with hepatic metastases: a case matched study. Eur J Surg Oncol 2010;36:365–70. [PubMed] DOI:10.1016/j.ejso.2009.11.007
- Thelen A, Jonas S, Benckert C, et al. Simultaneous versus staged liver resection of synchronous liver metastases from colorectal cancer. Int J Colorectal Dis 2007;22:1269–76. [PubMed] DOI:10.1007/s00384-007-0286-y