
Prognostic nutritional index is an independent prognostic factor for gastric cancer patients with peritoneal dissemination
Introduction
Gastric cancer is the fourth most common cancer and the third leading cause of cancer-related death worldwide (1). With early diagnosis, advances in surgery and standard chemotherapy, the overall survival (OS) of gastric cancer patients is increasing, particularly in Japan and Korea (2-4) However, most gastric cancer patients in China are diagnosed at an advanced stage (5).
Among the metastasis patterns of gastric cancer, peritoneal dissemination is the most common and lethal cause, which is considered the terminal period of gastric cancer (6). Gastric cancer patients with peritoneal dissemination often develop oral intake deficiency, overconsumption, bleeding, ascites and cancer pain, which cause debilitating malnutrition and immunological deterioration. Moreover, the worsened nutritional status can lead to development of the tumor by suppressing the immunity of the patients (7). Therefore, nutritional status plays a significant role in the OS of gastric cancer patients. Several studies demonstrated that various factors regarding the nutritional status are correlated with prognosis of gastric cancer patients (7-12). The prognostic nutritional index (PNI) is calculated by serum albumin and total lymphocyte count, including nutritional parameters and immune competence testing (13,14). It has been proposed as a simple and useful marker under the cutoff value of 45 to predict postoperative complication and the OS outcome after resection of gastric cancer and other malignancies (7,10,15-19).
Recently, Sachlova et al. reported that PNI represents a useful tool for evaluating the prognosis of patients with metastatic gastric cancer (12). However, the predictive and prognostic role of PNI in gastric cancer patients with peritoneal dissemination remains unclear. Therefore, the aim of this study was to explore the role of PNI in predicting the outcomes of gastric cancer patients with peritoneal dissemination.
Patients and methods
Patients
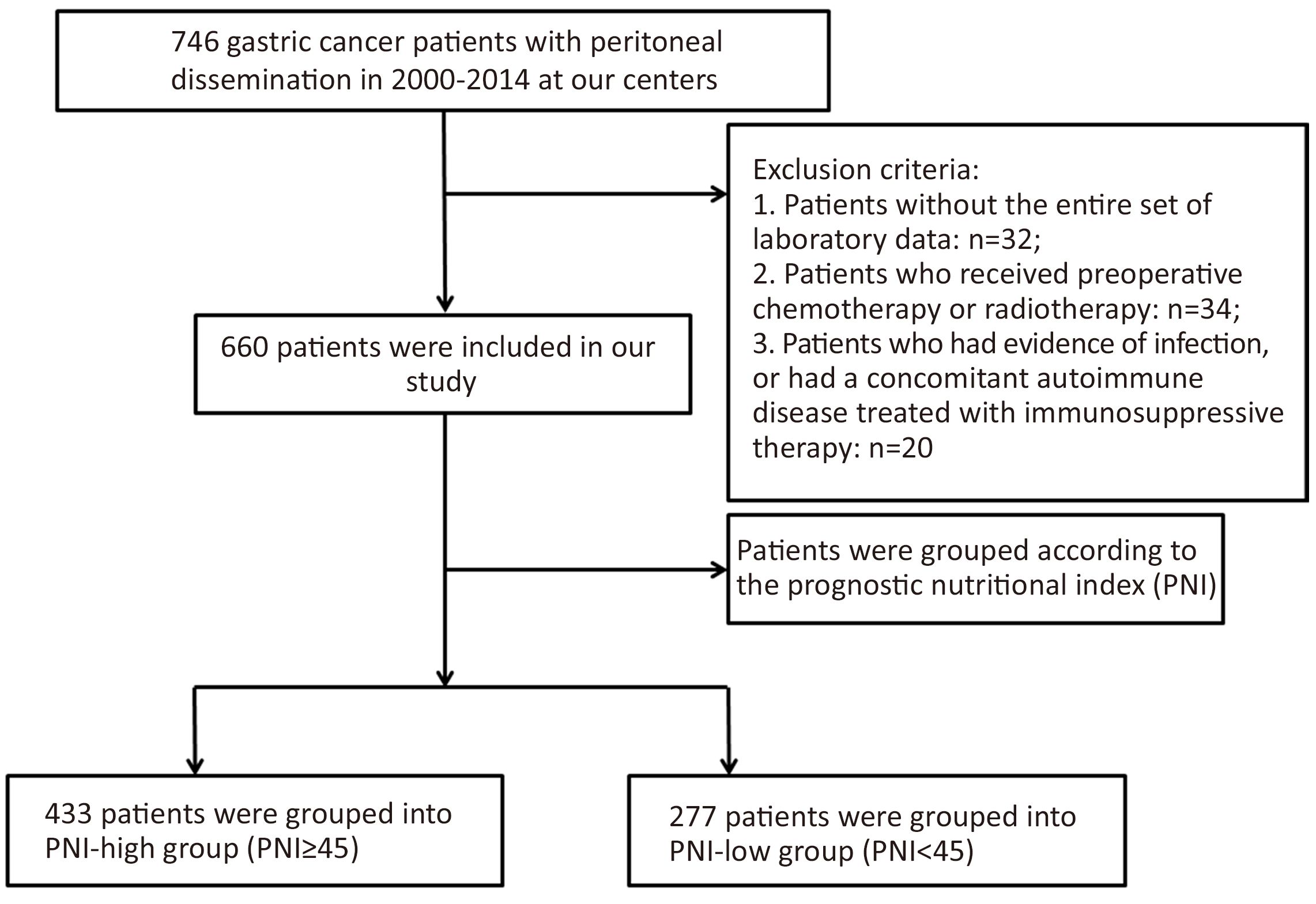
Between January 2000 and April 2014, a total of 660 patients were diagnosed with gastric adenocarcinoma with peritoneal metastasis at Sun Yat-sen University Cancer Center and the Sixth Affiliated Hospital of Sun Yat-sen University. The diagnosis of peritoneal dissemination was mainly through imaging test. Some patients were diagnosed with peritoneal dissemination by laparoscopic staging or laparotomy. The treatment, including palliative surgery and chemotherapy, was performed after obtaining written informed consent from all patients. The first-line chemotherapy regimens included a variety of agents, such as taxane, irinotecan, 5-fluorouracil, oxaliplatin and capecitabine. In the present study, postoperative morbidity was defined as the incidence rate of the postoperative complication and postoperative mortality was defined as death occurred in 30 d after operation. And this study was also approved by the independent Institute Research Ethics Committee at the Sun Yat-sen University Cancer Center and the Sixth Affiliated Hospital of Sun Yat-sen University. We conducted this retrospective research according to the principles expressed in the Declaration of Helsinki.
Information regarding patient demographics was collected for analysis. Only patients with an entire set of laboratory data were included in this study. Patients were excluded if they had evidence of infection, or a concomitant autoimmune disease treated with immunosuppressive therapy which affected their total lymphocyte count. Patients who received preoperative chemotherapy or radiotherapy were also excluded in this study (Figure 1).
Prognostic nutritional index (PNI)
The PNI was calculated as described previously using the following formula: 10× serum albumin concentration (g/dL) + 0.005× lymphocyte count (number/mm2) in peripheral blood (14). All nutritional factors were measured a few days before palliative surgery or first-line chemotherapy. The cutoff value in present study was set as 45, because PNIP<45 is defined as moderate to severe malnutrition. Therefore, the patients in this study were grouped into PNI-low group (PNIP<45) and PNI-high group (PNI≥45).
Statistical analysis
The categorical variables were presented as numbers and percentages, and Chi-square tests were used to compare categorical variables. OS was calculated from the diagnosis of peritoneal metastasis to death from any cause. Unadjusted Kaplan-Meier survival curves with log-rank testing were generated to compare the survival benefits. In the present study, median OS time was used to compare the survival benefits indirectly. Prognostic factors were analyzed by searching the clinicopathological factors in univariate analysis, and the variables with P<0.05 in the univariate analysis entered into multivariate analysis using Cox proportional hazard regression models. The forward selection method was used for multivariate Cox proportional analysis. The hazard ratio (HR) and 95% confidence interval (95% CI) were used to estimate the role of each predictor of survival. Two-sided P<0.05 was considered statistically significant. All of the above statistical analyses were performed by SPSS software (version 17.0; SPSS Inc., Chicago, IL, USA).
All of the regular follow-up assessments were completed by November 2015, and the median follow-up was 12.3 months (range, 0.3−56.1 months).
Results
Patient characteristics
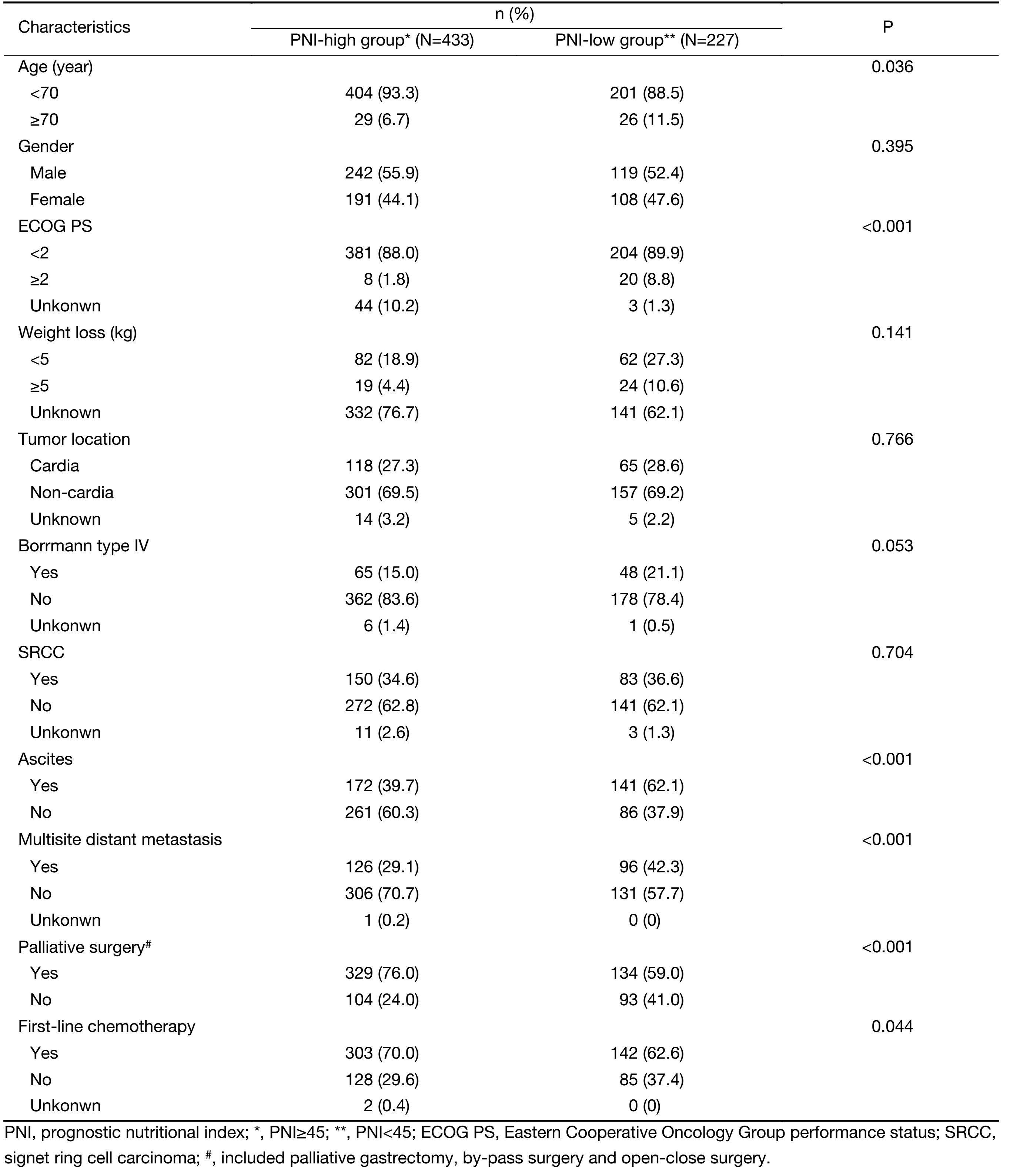
The baseline characteristics of 660 gastric cancer patients with peritoneal dissemination are shown in Table 1. There were 433 patients in the PNI-high group and 227 patients in the PNI-low group. Compared with PNI-high group, PNI-low group was likely to be older (11.5% vs. 6.7%, P=0.036), to have worse performance status (PS) (8.8% vs. 1.8%, P<0.001), higher frequency of ascites (62.1% vs. 39.7%, P<0.001), higher frequency of multisite distant metastasis (42.3% vs. 29.1%, P<0.001), less palliative surgery (59.0% vs. 76.0%, P<0.001) and first-line chemotherapy (62.6% vs. 70.0%, P=0.044). The other baseline characteristics between the two groups had no difference.
Full table
Overall survival
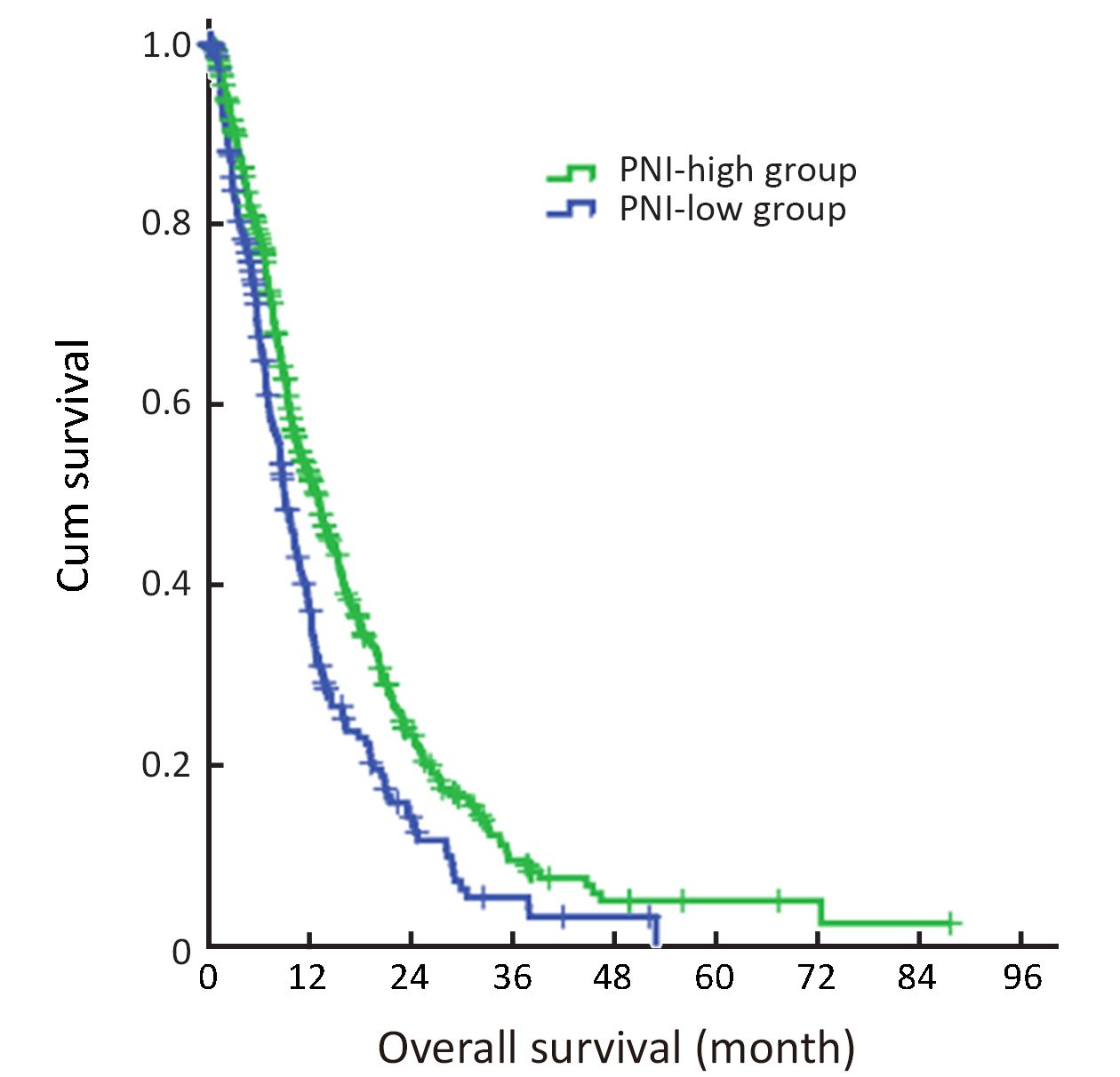
The median OS was 13.13 (95% CI, 11.35−14.92) months in the PNI-high group and 9.03 (95% CI, 7.85−10.22) months in the PNI-low group (Figure 2). The OS difference between the groups was significant (P<0.001).
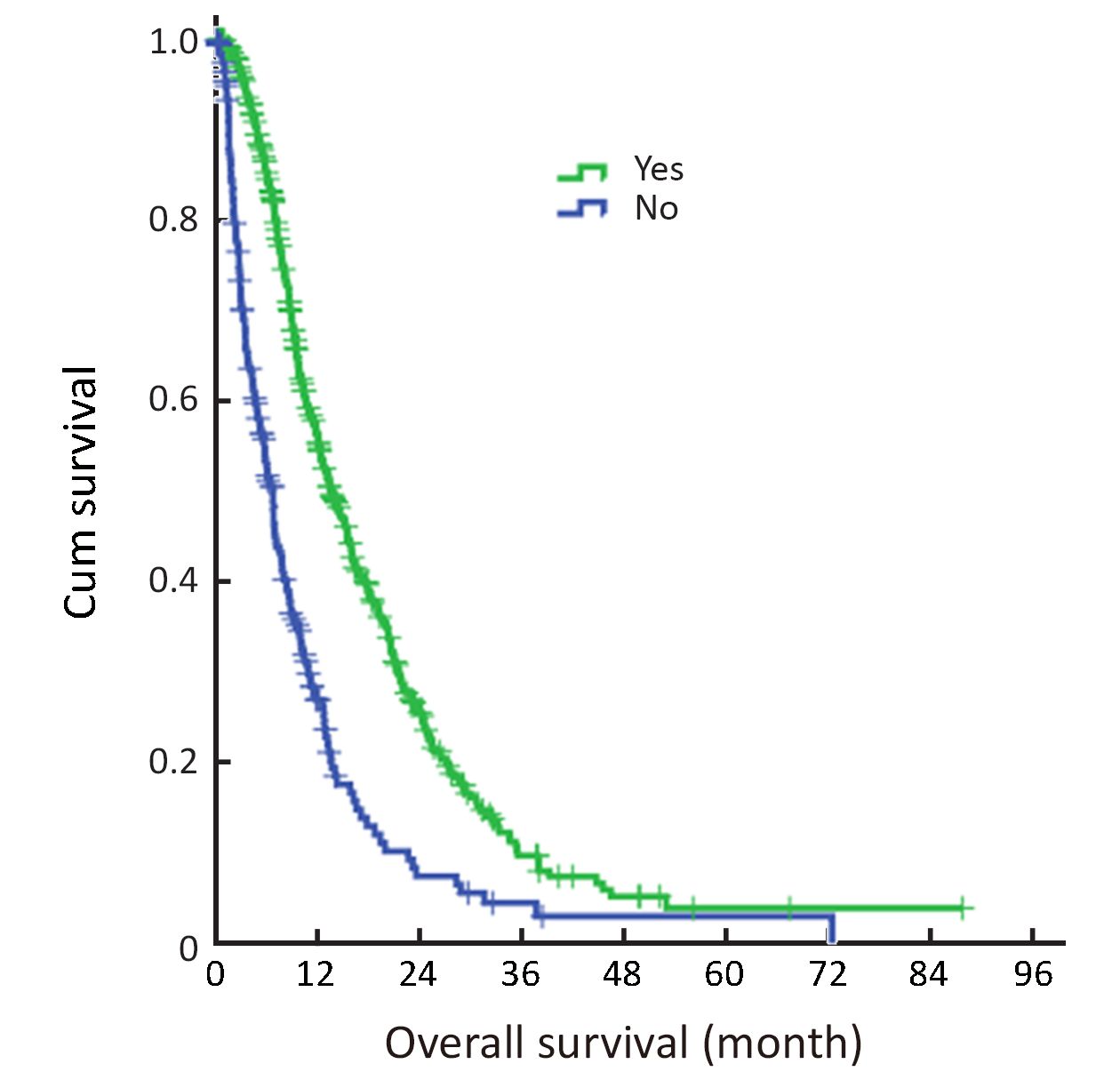
Patients receiving first-line chemotherapy had a significantly longer median OS of 13.57 (95% CI, 11.91−15.23) months compared with 6.70 (95% CI, 5.76−7.64) months in patients who did not (P<0.001) (Figure 3).
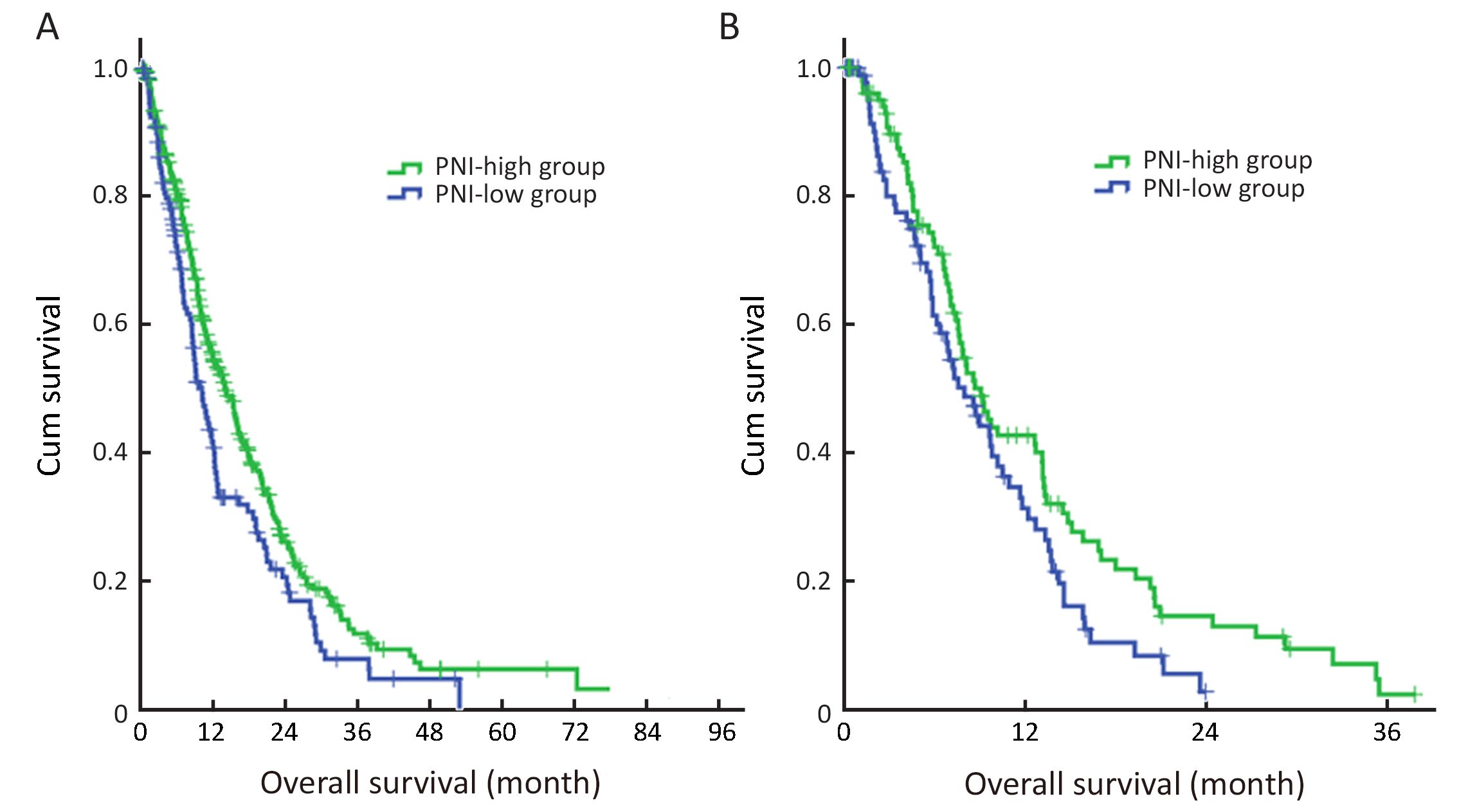
In the subgroup analysis, for patients receiving palliative surgery, patients in the PNI-high group had a significantly longer median OS than patients in the PNI-low group [14.03 (95% CI, 11.80−16.26) months vs. 10.13 (95% CI, 8.20−12.06) months; P=0.009] (Figure 4A). However, for patients not receiving palliative surgery, the median OS between PNI-high and PNI-low groups was not significantly different [9.07 (95% CI, 7.42−10.72) months vs. 7.97 (95% CI, 5.92−10.01) months; P=0.051] (Figure 4B).
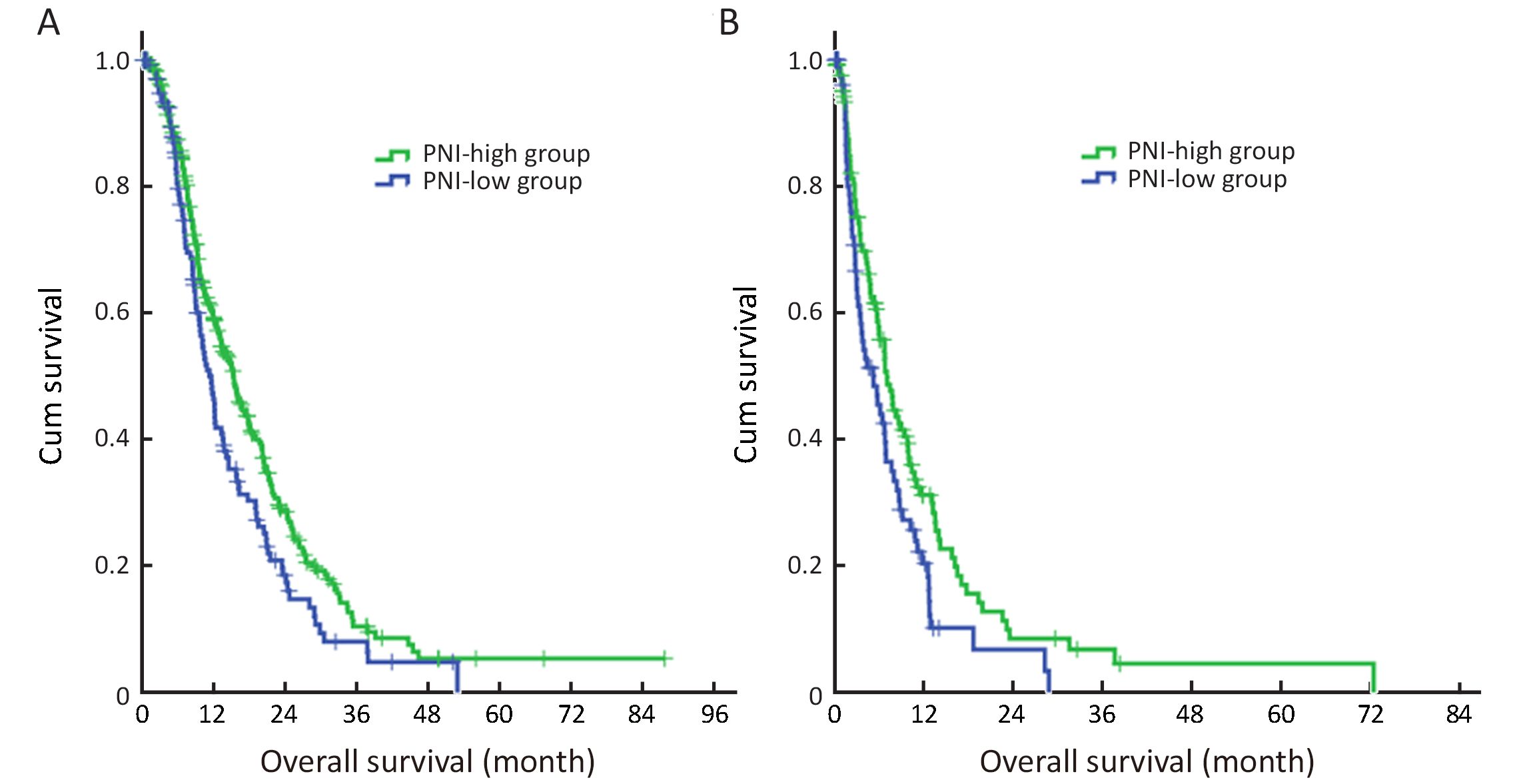
The median OS in the PNI-high group was significantly longer than that in the PNI-low group both for patients receiving first-line chemotherapy [15.40 (95% CI, 13.33−17.47) months vs. 11.67 (95% CI, 9.95−13.39) months; P=0.010] (Figure 5A) and patients not receiving first-line chemotherapy [7.03 (95% CI, 5.49−8.58) months vs. 5.20 (95% CI, 2.81−7.59) months; P=0.019] (Figure 5B).
Univariate and multivariate analysis for OS
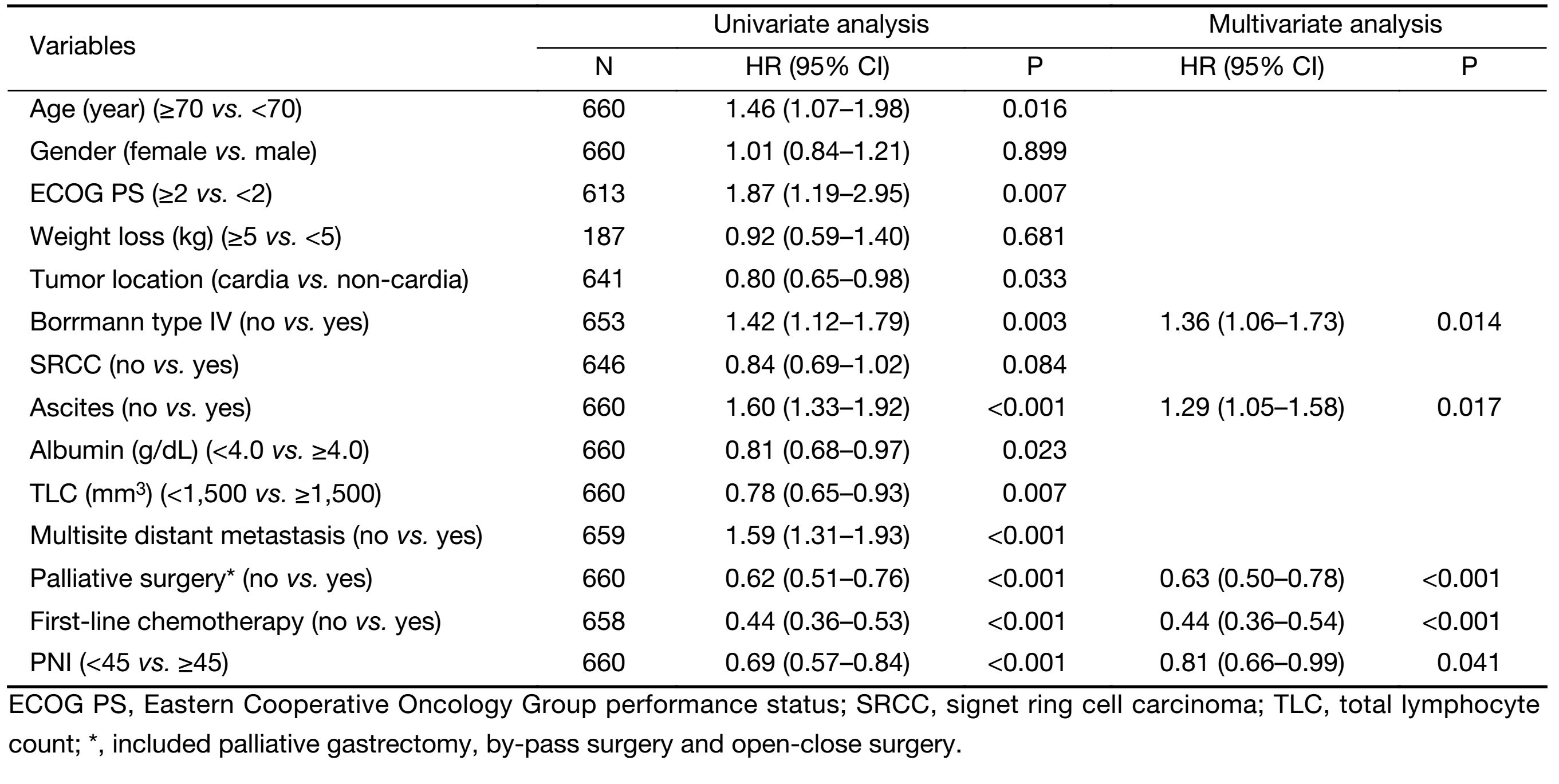
In univariate analysis, age (P=0.016), PS (P=0.007), tumor location (P=0.033), Borrmann type IV (P=0.003), ascites (P<0.001), serum albumin (P=0.023), serum total lymphocyte count (P=0.007), multisite distant metastasis (P<0.001), palliative surgery (P<0.001), first-line chemotherapy (P<0.001) and PNI (P<0.001) were significant predictors of OS (Table 2). Multivariate survival analysis demonstrated that Borrmann type IV (P=0.014), presence of ascites (P=0.017) and lower PNI (P=0.041) remained independent poor prognostic factors, and palliative surgery (P<0.001) and first-line chemotherapy (P<0.001) were good prognostic factors (Table 2).
Full table
Postoperative morbidity and mortality
For patients receiving palliative surgery, there was no significant difference between PNI-low group and PNI-high group regarding the postoperative morbidity rate, which were 9.0% (12/134) and 9.7% (32/329), respectively (P=0.797). PNI-low group had a higher postoperative mortality rate of 2.2% (3/134), compared with 0.9% (3/329) in the PNI-high group; however, the difference was not significant (P=0.252).
Discussion
With a 5-year OS less than 2%, peritoneal dissemination is considered the terminal period of gastric cancer (20). Malnutrition often tortures gastric cancer patients with peritoneal dissemination, which decreases the patients’ quality of life. Moreover, immunological and nutritional disorder can cause a decline in serum albumin concentration, total lymphocyte count (TLC), helper T cells, interleukins 2 and 3, and T cell blastogenic responses (7). In the present study, we noted that lower PNI, a simple inflammation-based prognostic score, was correlated significantly with advanced age, higher frequency of ascites and multisite distant metastasis, suggesting that lower PNI is correlated with a more aggressive disease phenotype. Univariate and multivariate analysis also demonstrated that PNI was an independent predictor of OS in gastric cancer patients with peritoneal dissemination, especially for patients who need to receive palliative surgery to relieve cancer-related symptoms, such as tumor bleeding, obstruction and perforation. Our results were also supported by other studies (11,21).
Until now, various indexes have been offered to assess the nutritional status in cancer patients (8,9,22,23). All the assessment indexes have their own merits, but they have also raised a series of questions. PS is a direct index to reflect the nutritional status of the patients, which is considered to be a significant prognostic factor. However, the PS assessment may be subjective and biased. In our study, multivariate analysis demonstrated that PNI is superior to PS in terms of prognostic ability.
Lien et al. reported that preoperative serum albumin level was correlated highly with resectability and survival in gastric cancer patients (8). Serum albumin is not only a window to recognize the nutritional status of the patients but also a useful tool for predicting the prognostic outcome of cancer patients. However, serum albumin has its own defect in predicting the prognostic outcome of the cancer patients. First, serum albumin has a long half-life period of 20 days, and therefore cannot reflect the short-term nutrition state of the patients; second, serum albumin is easily influenced by non-nutritional factors, such as acute phase reaction, the hydration status of patients, renal function, liver function and extravascular fluid alteration. According to the multivariate analysis of our study, serum albumin did not reflect patients’ outcome. Bruckner et al. reported that total lymphocyte count was an independent prognostic factor for patients with advanced gastric cancer (23). However, the multivariate analysis of our study showed that total lymphocyte count was not an indepen-dent prognostic factor. This indicated that total lymphocyte count was not an effective factor to predict the survival outcome of the gastric patients with peritoneal dissemination. Just as serum albumin, there may be lots of impacts influencing the PNI, too; nevertheless, our results revealed that PNI, the combination of serum albumin and total lymphocyte count, showed preponderance in predicting the outcome of gastric cancer patients with peritoneal dissemination.
Although the final results of the Regatta trial showed that palliative gastrectomy combined with chemotherapy was not superior to chemotherapy alone for advanced gastric cancer patients with a single non-curable factor (24), palliative surgery was still important for patients experiencing cancer-related symptoms, such as tumor bleeding, obstruction and perforation. The postoperative morbidity and mortality were acceptable (25). However, our results demonstrated that PNI was not a predict factor regarding postoperative complication and mortality, which was contradiction to other studies (18,26). Therefore, this indicated that PNI of gastric cancer patients with peritoneal dissemination was a prognostication of OS, but not for postoperative morbidity and mortality.
Theoretically, gastric cancer patients with malnutrition can benefit from correction of preoperative immuno-nutritional disorders through intravenous infusion of albumin and parenteral nutrition, but it lacks clinical trials to confirm. Qiu et al. reported that nutrition improvement after nutrition support indicated a survival benefit for stage IV gastric cancer patients (27). Unfortunately, their study also showed that only 30.3% of patients had the nutritional improvement after nutrition support. Furthermore, it remains unclear whether a low PNI is a cause or a consequence of tumor progression (11). In the future, well-designed large scale randomized controlled clinical trials on the value of management in the PNI-low group are required.
This study is a substantially retrospective study with several missed data of clinicopathological characteristics of the enrolled patients, which is a potential limitation of this study. Although the data in our study were from two high-volume institutions, the results of this study should be interpreted cautiously. A large-scale prospective validation study is required to confirm the results.
Conclusions
The present study indicated that PNI is a useful and practical tool for evaluating the nutritional status of gastric cancer patients with peritoneal dissemination, and is also an independent prognostic factor of OS for these patients.
Acknowledgements
Funding: This work was supported in part by a grant from National Natural Science Foundation of China (No. 81302144) and the Guangdong Science and Technology Department (No. 2012B061700087).
Footnote
Conflicts of Interest: The authors have no conflicts of interest to declare.
References
- Torre LA, Bray F, Siegel RL, et al. Global cancer statistics, 2012. CA Cancer J Clin 2015;65:87–108. [PubMed] DOI:10.3322/caac.21262
- Songun I, Putter H, Kranenbarg EM, et al. Surgical treatment of gastric cancer: 15-year follow-up results of the randomised nationwide Dutch D1D2 trial. Lancet Oncol 2010;11:439–49. [PubMed] DOI:10.1016/S1470-2045(10)70070-X
- Sasako M, Sakuramoto S, Katai H, et al. Five-year outcomes of a randomized phase III trial comparing adjuvant chemotherapy with S-1 versus surgery alone in stage II or III gastric cancer. J Clin Oncol 2011;29:4387–93. [PubMed] DOI:10.1200/JCO.2011.36.5908
- Bang YJ, Kim YW, Yang HK, et al. Adjuvant capecitabine and oxaliplatin for gastric cancer after D2 gastrectomy (CLASSIC): a phase 3 open-label, randomised controlled trial. Lancet 2012;379:315–21. [PubMed] DOI:10.1016/S0140-6736(11)61873-4
- Chen S, Li YF, Feng XY, et al. Significance of palliative gastrectomy for late-stage gastric cancer patients. J Surg Oncol 2012;106:862–71. [PubMed] DOI:10.1002/jso.23158
- Hioki M, Gotohda N, Konishi M, et al. Predictive factors improving survival after gastrectomy in gastric cancer patients with peritoneal carcinomatosis. World J Surg 2010;34:555–62. [PubMed] DOI:10.1007/s00268-010-0396-5
- Kanda M, Fujii T, Kodera Y, et al. Nutritional predictors of postoperative outcome in pancreatic cancer. Br J Surg 2011;98:268–74. [PubMed] DOI:10.1002/bjs.v98.2
- Lien YC, Hsieh CC, Wu YC, et al. Preoperative serum albumin level is a prognostic indicator for adenocarcinoma of the gastric cardia. J Gastrointest Surg 2004;8:1041–8. [PubMed] DOI:10.1016/j.gassur.2004.09.033
- Mohri Y, Tanaka K, Ohi M, et al. Prognostic significance of host- and tumor-related factors in patients with gastric cancer. World J Surg 2010;34:285–90. [PubMed] DOI:10.1007/s00268-009-0302-1
- Nozoe T, Ninomiya M, Maeda T, et al. Prognostic nutritional index: a tool to predict the biological aggressiveness of gastric carcinoma. Surg Today 2010;40:440–3. [PubMed] DOI:10.1007/s00595-009-4065-y
- Eo WK, Chang HJ, Suh J, et al. The prognostic nutritional index predicts survival and identifies aggressiveness of gastric cancer. Nutr Cancer 2015;67:1260–7. [PubMed] DOI:10.1080/01635581.2015.1082112
- Sachlova M, Majek O, Tucek S. Prognostic value of scores based on malnutrition or systemic inflamma-tory response in patients with metastatic or recurrent gastric cancer. Nutr Cancer 2014;66:1362–70. [PubMed] DOI:10.1080/01635581.2014.956261
- Buzby GP, Mullen JL, Matthews DC, et al. Prognostic nutritional index in gastrointestinal surgery. Am J Surg 1980;139:160–7. [PubMed] DOI:10.1016/0002-9610(80)90246-9
- Onodera T, Goseki N, Kosaki G. Prognostic nutritional index in gastrointestinal surgery of malnourished cancer patients. Nihon Geka Gakkai Zasshi (in Japanese) 1984;85:1001–5. [PubMed]
- Kinoshita A, Onoda H, Imai N, et al. Comparison of the prognostic value of inflammation-based prognostic scores in patients with hepatocellular carcinoma. Br J Cancer 2012;107:988–93. [PubMed] DOI:10.1038/bjc.2012.354
- Nozoe T, Kohno M, Iguchi T, et al. The prognostic nutritional index can be a prognostic indicator in colorectal carcinoma. Surg Today 2012;42:532–5. [PubMed] DOI:10.1007/s00595-011-0061-0
- Pinato DJ, North BV, Sharma R. A novel, externally validated inflammation-based prognostic algorithm in hepatocellular carcinoma: the prognostic nutritional index (PNI). Br J Cancer 2012;106:1439–45. [PubMed] DOI:10.1038/bjc.2012.92
- Watanabe M, Iwatsuki M, Iwagami S, et al. Prognostic nutritional index predicts outcomes of gastrectomy in the elderly. World J Surg 2012;36:1632–9. [PubMed] DOI:10.1007/s00268-012-1526-z
- Jiang N, Deng JY, Ding XW, et al. Prognostic nutritional index predicts postoperative complications and long-term outcomes of gastric cancer. World J Gastroenterol 2014;20:10537–44. [PubMed] DOI:10.3748/wjg.v20.i30.10537
- Bando E, Yonemura Y, Takeshita Y, et al. Intraoperative lavage for cytological examination in 1,297 patients with gastric carcinoma. Am J Surg 1999;178:256–62. [PubMed] DOI:10.1016/S0002-9610(99)00162-2
- Sakurai K, Ohira M, Tamura T, et al. Predictive potential of preoperative nutritional status in long-term outcome projections for patients with gastric cancer. Ann Surg Oncol 2016;23:525–33. [PubMed] DOI:10.1245/s10434-015-4814-7
- Eo WK, Jeong DW, Chang HJ, et al. Absolute monocyte and lymphocyte count prognostic score for patients with gastric cancer. World J Gastroenterol 2015;21:2668–76. [PubMed] DOI:10.3748/wjg.v21.i9.2668
- Bruckner HW, Lavin PT, Plaxe SC, et al. Absolute granulocyte, lymphocyte, and moncyte counts. Useful determinants of prognosis for patients with metastatic cancer of the stomach. JAMA 1982(247):1004–6. [PubMed]
- Fujitani K, Yang HK, Mizusawa J, et al. Gastrectomy plus chemotherapy versus chemotherapy alone for advanced gastric cancer with a single non-curable factor (REGATTA): a phase 3, randomised controlled trial. Lancet Oncol 2016;17:309–18. [PubMed] DOI:10.1016/S1470-2045(15)00553-7
- Nie RC, Chen S, Yuan SQ, et al. Significant role of palliative gastrectomy in selective gastric cancer patients with peritoneal dissemination: a propensity score matching analysis. Ann Surg Oncol 2016;23:3956–63. [PubMed] DOI:10.1245/s10434-016-5223-2
- Sun K, Chen S, Xu J, et al. The prognostic significance of the prognostic nutritional index in cancer: a systematic review and meta-analysis. J Cancer Res Clin Oncol 2014;140:1537–49. [PubMed] DOI:10.1007/s00432-014-1714-3
- Qiu M, Zhou YX, Jin Y, et al. Nutrition support can bring survival benefit to high nutrition risk gastric cancer patients who received chemotherapy. Support Care Cancer 2015;23:1933–9. [PubMed] DOI:10.1007/s00520-014-2523-6