
Comprehensive evaluation of nutritional status before and after hematopoietic stem cell transplantation in 170 patients with hematological diseases
Introduction
In recent years, hematopoietic stem cell transplantation (HSCT) has been widely used as a primary treatment for malignant cancers of blood system and some solid tumors (1). Patients with hematological diseases must receive multiple high-dose chemical and/or systemic radiation treatments prior to transplantation, which often leads to digestive dysfunctions that cause moderate to severe malnutrition in patients at nutritional risk. Good nutrition is significant for immune and bone marrow reconstitution following HSCT (2). Whether the nutritional status of patients before and during HSCT affects immune reconstitution after transplantation is of great concern to the clinicians, patients and their relatives. Therefore, an accurate and timely nutritional assessment of the patients with hematological diseases, before and after transplantation, is critical to develop a nutritional support regimen and assure successful completion of HSCT, immune reconstitution after transplantation, reduced risks of infection and graft-versus-host disease, and increased quality of life.
By now, there are few studies on nutritional assessment of hematological patients before and after HSCT, and additionally, most rely on one single assessment method. Nutritional risk screening and assessment tools widely used in clinic include Nutritional Risk Screening 2002 (NRS-2002), Mini Nutritional Assessment (MNA), Subjective Global Assessment (SGA) and Malnutrition Universal Screening Tools (MUST), etc. Due to the particularity of blood cancer treatments, all the above assessment tools have obvious limitations such as low specificity, and low detection and predictive values as a singular nutritional screening and assessment method (3-5). Therefore, this study will use these four methods, in combination with body measurements, to assess the nutritional status of patients with hematological diseases before and after HSCT, and prospectively, aim to explore the best assessment regimen and provide theoretical and scientific basis for the nutrition therapy of patients with hematological diseases.
Patients and methods
Patients
This cohort study enrolled 170 patients who were diagnosed with hematological diseases and underwent allogeneic HSCT in the Department of Hematology, Peking University People's Hospital between May 2011 and April 2013. The cohort, including 116 males and 54 females, with a median age of 30 (range, 12–56) years, comprised 63 cases of acute lymphocytic leukemia (ALL), 65 acute myeloid leukemia (AML), 14 chronic myeloid leukemia (CML), 22 myelodysplastic syndrome (MDS), 3 lymphoma and 3 aplastic anemia. This study was reviewed and approved by the Ethical Committee of Peking University People's Hospital. Informed consent was obtained from all the patients.
The inclusion criteria included: 1) patients who were diagnosed with hematological diseases and would receive HSCT at the Department of Hematology, Peking University People's Hospital; 2) age ≥6 years old; 3) without severe heart, liver, brain, or kidney failure; 4) did not participate in other clinical trials within 4 weeks; and 5) signed informed consent.
The exclusion criteria included: 1) patients diagnosed with acute promyelocytic leukemia (APL); 2) patients suffering from malignant tumors other than blood diseases; 3) chronic hepatitis or cirrhosis; 4) serum aspartate aminotransferase (AST) ≥1.5 times the upper limit of normal (ULN) or alanine aminotransferase (ALT) ≥1.5 times ULN; 5) recent or large abdominal surgery such as gastrectomy (surgeries without long-term side effects, such as appendectomy, cholecystectomy, polypectomy, etc., may not be excluded); 6) infectious diseases such as human immunodeficiency virus (HIV) and active tuberculosis; 7) poorly controlled hypertension; or 8) pregnant or lactating women.
Nutritional assessment methods
Using fixed-point continuous sampling, all patients received nutritional assessment by four methods (NRS-2002, MNA, SGA and MUST), in combination with body measurements, before entering laminar air flow rooms for HSCT and after leaving laminar air flow rooms.
Human body measurements
Height, weight, waist circumference (WC), hip circumference (HC) and hand grip strength were measured routinely (6,7). Body mass index (BMI) and waist-hip ratio (WHR) were calculated according to the following formulas: BMI = body weight (kg)/[height (m)]2 and WHR = WC/HC. Skinfold thickness measurements included triceps skinfold thickness (TSF), subscapular skinfold thickness (SSF), and suprailiac skinfold thickness. The average daily water intake was recorded in a scale.
Nutritional risk screening and assessment
Assessment method of NRS-2002 was developed by the Danish Association of Parenteral and Enteral Nutrition (DAPEN), and was recommended by the European Society for Clinical Nutrition and Metabolism (ESPEN). This method was established on evidence-based medicine and was easy to implement. The core issues include: 1) the severity of the effect of primary disease on nutritional status; 2) recent (1 to 3 months) changes in body weight; 3) dietary intake changes in the most recent week; 4) BMI; and 5) an extra score point is added to the nutritional risk score of patients ≥70 years. Nutritional risk is assessed by the scoring method, and a score of ≥3 was used as a criterion for the presence of nutritional risk. Considering the differences in height and weight between the Eastern and Western populations, the assessment of BMI is according to the classification recommended by Chunming Chen for Chinese adults (8), wherein the adult malnutrition criteria are: BMI <18.5 kg/m2 for nutritional deficiencies, BMI ≥24.0 kg/m2 for overweight and BMI ≥28.0 kg/m2 for obesity.
In the early 1990s, Vellas et al. developed a new method, MNA, for the assessment of human nutritional status (9,10). MNA questionnaire consists of 18 items in four categories, 30 points in total. MNA score ≥24 indicates normal nutritional status; 17≤ MNA score ≤23.5 indicates a potential risk of malnutrition; MNA score <17 is considered as malnourished.
SGA was proposed by Canadian scholars as a clinical nutritional evaluation method in 1981, and was recommended by the American Society for Parenteral and Enteral Nutrition (ASPEN). SGA assessment is based on medical history and clinical examination, and includes 8 indicators: weight changes, dietary intake, gastrointestinal symptoms, functional capacity evaluation, stress, muscle wasting, TSF and the presence of edema. Each indicator is divided into three grades: A, B and C (11). When there are 5 or more C-grades among the 8 indicators, the overall rating is C (severe malnourishment); with 5 or more B-grades, or some C-grades but less than 5, the overall rating is B (mild to moderate malnourishment); when the B-and C-grades are less than 5, the overall rating is A (normal nutrition). The evaluation of low, moderate and severe stress (corresponding to A, B, C levels) is based on the mental status of patients after bone marrow trans-plantation. If low mood or depression with tendency of mental disorders is evident, the stress level is C (severe stress), otherwise, recorded as B (moderate stress) due to the expected stress from the transplantation procedure.
MUST method was developed by the British Association for Parenteral and Enteral Nutrition (BAPEN). It is primarily used for screening protein-energy malnutrition and its incidence risk, including estimation of the following three criteria: BMI, body weight loss and disease-induced food intake reduction (12,13). Total score is equal to the sum of the three criteria. Score 0 represents no or low nutritional risk, indicating that a replicate screening may be required after a certain time interval. Score 1 represents moderate nutritional risk, indicating that food intake should be monitored for 3 d and recorded for further evaluation. Score 2 represents high nutritional risk, indicating that patients should be referred to a dietitian for nutrition guidance or therapy.
Quality control
All the patients were evaluated on the day they entered the laminar air flow room for HSCT, and 109 were evaluated on the day they left the room because 61 patients could not be evaluated due to some unexpected circumstances and were therefore excluded. Two experienced dietitians performed the evaluation. A uniform dietary survey was used for screening and evaluation. Patients' height was measured without shoes; body weight was measured under fasting condition with hospital gown and without shoes, using a body-weight scale (RGZ-120, Changzhou Wujin Weighing Apparatus Co., Ltd, China). The grip strength was measured with a hand-dynamometer (EH101, Guangdong Senssun Weighing Apparatus Group Ltd., China). Height measurement error adjustment was ±0.5 cm and body weight measurement error adjustment was ±0.2 kg. Skinfold thickness was measured by a skinfold caliper manufactured by the China National Sports Commission, and body circumferences were measured using a standard flexible ruler with an accuracy of 0.1 mm.
Statistical analysis
All data were imported and managed using Epi-Data software program (the EpiData Association, Denmark). Statistical analysis was performed using SPSS software version 18.0 (SPSS Inc., Chicago, IL, USA). Measurement data were expressed as x±s, and analyzed by paired t-test. Enumeration data were expressed as percentages, and analyzed by the Pearson's Chi-squared test. P<0.05 was considered statistically significant.
Results
All patients received nutritional assessment on the day of entering laminar air flow room; 109 patients received the nutritional assessment within 48 h after leaving laminar air flow room; and 102 patients participated in the human body measurements both before and after transplantation. Mean laminar air flow room treatment time was 30.0±2.1 d.
Anthropometry
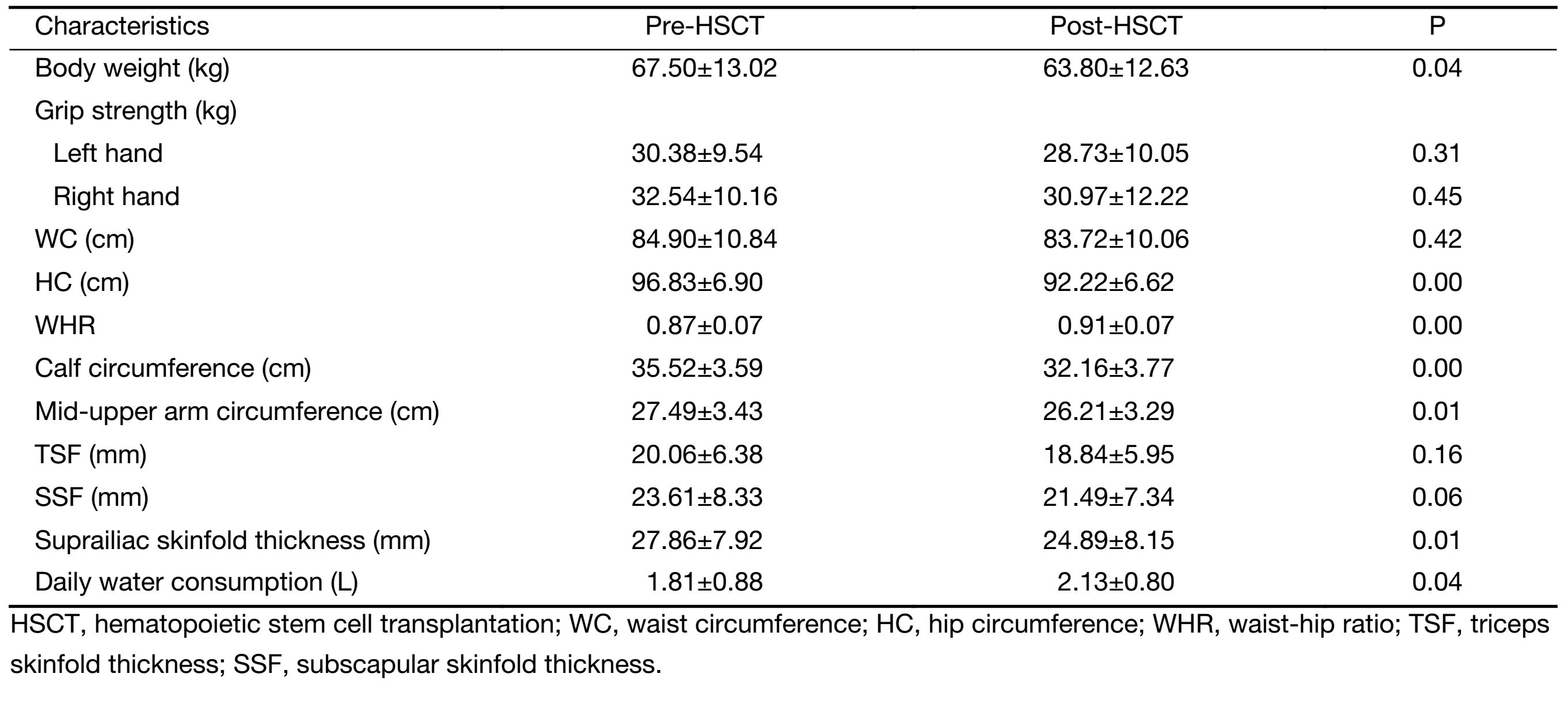
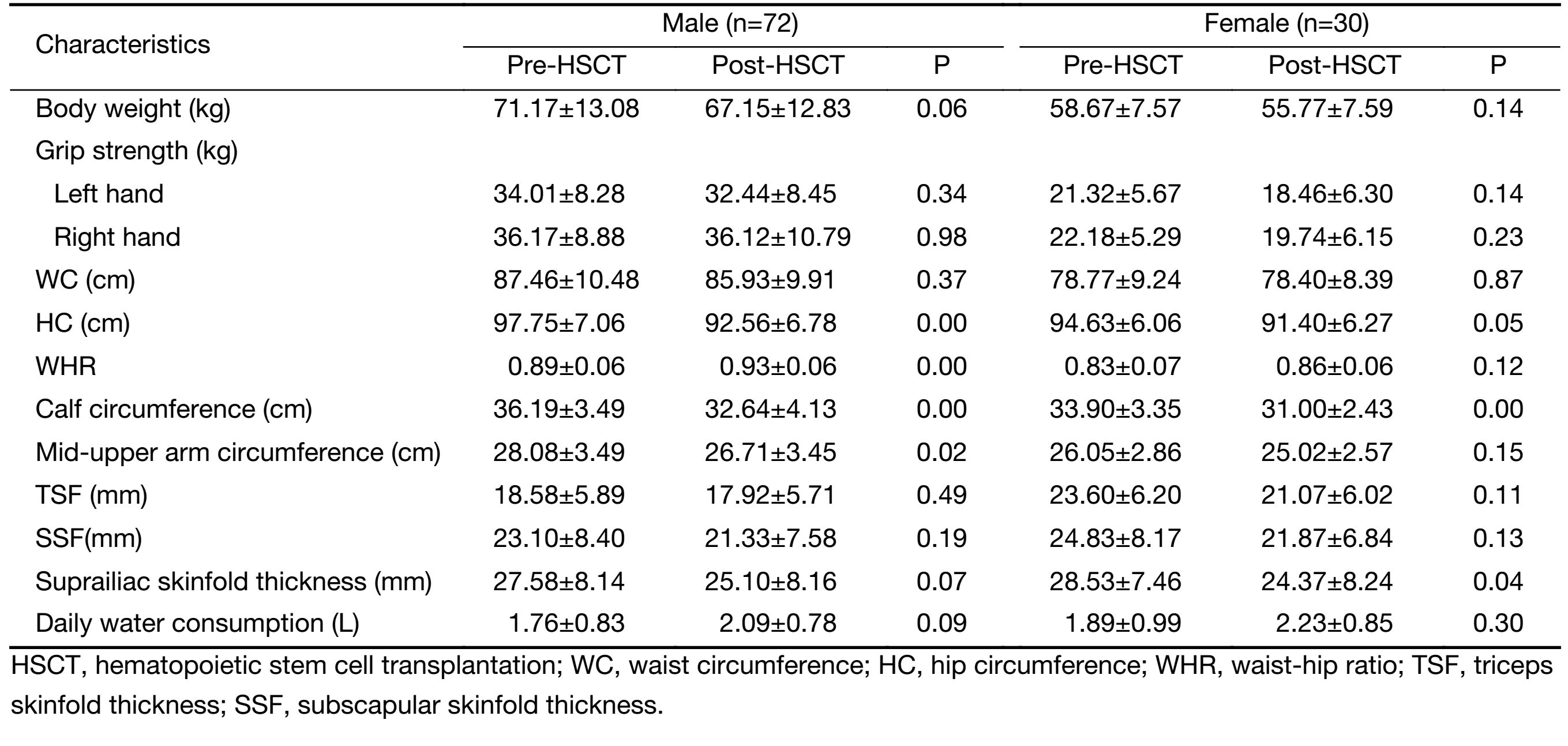
The height of patients was 1.69±0.08 m, wherein the male was 1.73±0.07 m, and the female was 1.62±0.05 m. The body weight and grip strength of patients pre- and post-transplantation are shown in Table 1 and Table 2. The results showed that the body weight, HC, WHR, calf circumference, mid-upper arm circumference and suprailiac skinfold thickness of the patients decreased dramatically after transplantation. The average body weight loss was 4 kg and 3 kg for males and females, respectively, although there was no statistical significance. The grip strength of both hands, WC, TSF and SSF did not show obvious changes. After transplantation, daily water intake increased significantly, and HC and mid-upper arm circumference decreased slightly, but there was no statistical significance.
Full table
Full table
NRS-2002 evaluation
Before HSCT, only 36 cases among the total patients involved in this study had nutritional risk, but all the 109 patients evaluated after HSCT had nutritional risk, wherein 29 (26.6%) got a score of 3, 13 (11.9%) scored 4–5, and 67 (61.5%) scored 6. All patients involved in this study got a score of 3 for the item of "severity of the impact of primary diseases on nutritional status". Fifty-five patients (50.5%) lost more than 5% of their body weight during treatment in the laminar air flow room. Twenty-six (23.9%) showed a reduction in food intake (60% less than pre-HSCT), while 19 (17.4%) showed increased food intake than before.
MNA evaluation
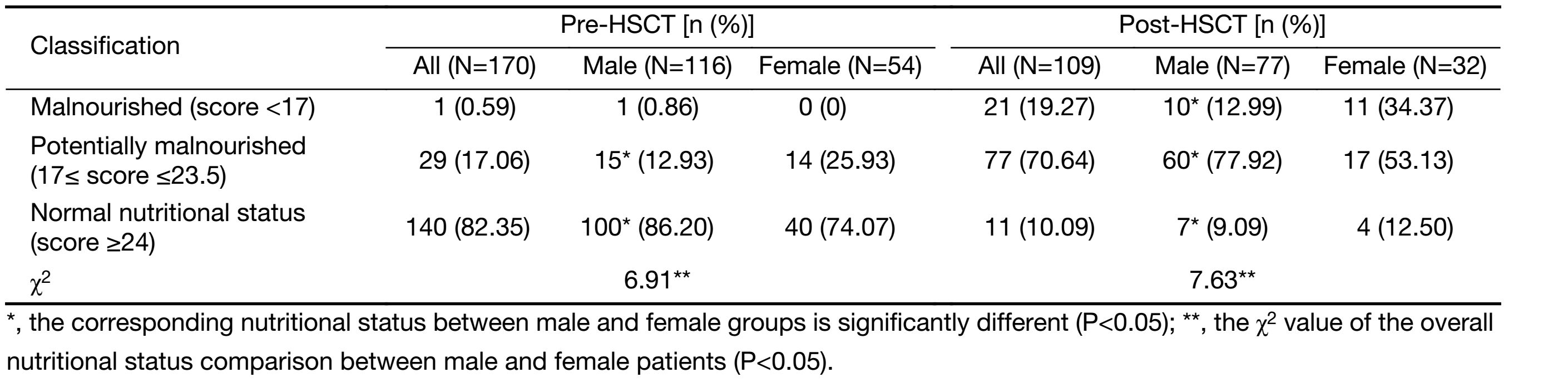
Before HSCT, most patients with hematological diseases had good nutritional status. Males showed better nutritional status than females; 86.20% of the males had good nutritional status, while 74.07% for the females. After HSCT, only 10.09% of the patients had good nutritional status, and 70.64% of the patients showed potential malnutrition. As shown in Table 3, the percentage of malnutrition for females after HSCT was significantly higher than that for males.
Full table
SGA evaluation
Among 170 patients, before transplantation, there were no patients with severe malnutrition and only 3 (1.76%) had moderate malnutrition. The rest had normal nutritional status. After HSCT, 90 patients (82.6%) developed moderate or severe malnutrition. Among those, no female patients suffered from severe malnutrition, while 27 females (84.4%) had moderate malnutrition; 63 male patients (81.8%) developed moderate or severe malnutrition, wherein only one had severe malnutrition. After transplantation, 87.1% of patients experienced muscle wasting, among which, 9.3% had severe muscle wasting. The results from assessment of TSF were consistent with muscle wasting.
MUST evaluation
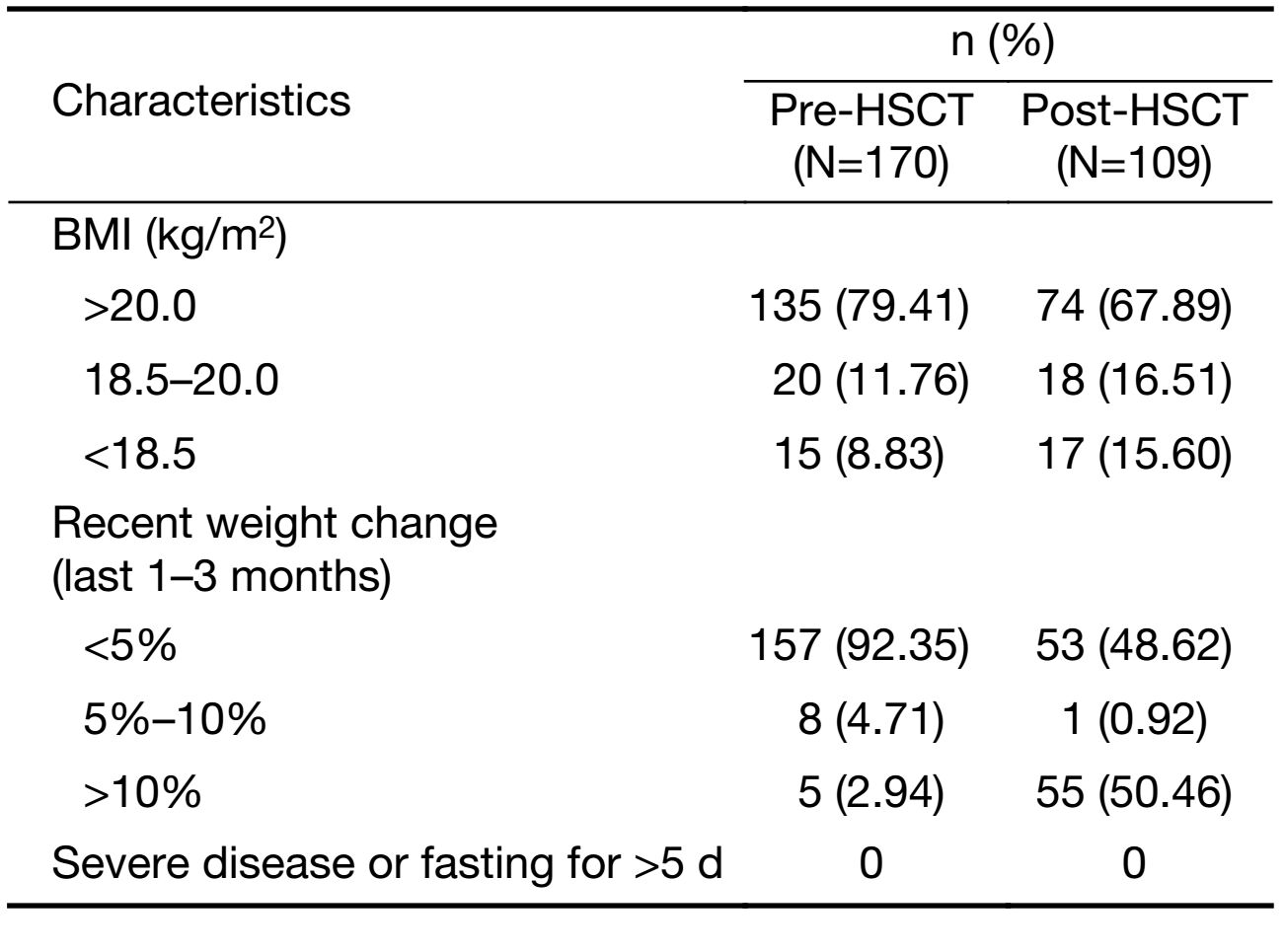
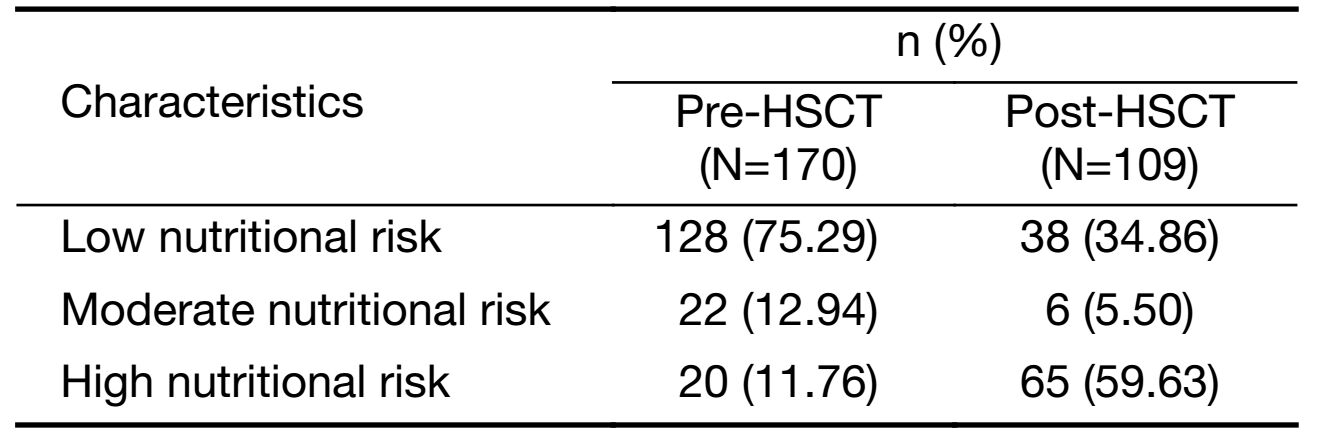
Before and after transplantation, no patient developed other severe diseases or complications, and no patient experienced fasting for more than 5 d. Before transplantation, only 2.94% of all patients had recent weight loss of more than 10%, while 55 patients (50.46%) experienced weight loss of more than 10% during treatment in the laminar air flow room (Table 4). MUST evaluation showed that 20 patients (11.76%) had high nutritional risk before transplantation, and after HSCT, 65 patients (59.63%) had high nutritional risk (Table 5).
Full table
Full table
Discussion
Domestic and foreign literature shows that 25%–60% of hospitalized patients suffer from malnutrition (14,15). In clinical practice, nutritional support and nutrition therapy are always delayed. Although doctors understand the importance of nutrition in the course of treatment, intervention is rare in patients without severe malnutrition or capable of self-feeding. In case severe malnutrition, cachexia, graft-versus-host disease, oral ulcers, infections and other complications occur, patients begin to receive nutrition therapy. However, due to poor implementation, the survival rate and quality of life of patients are seriously affected. Therefore, treatment of patients with hematological diseases should initiate from the correct nutritional evaluation.
In this study, before transplantation, the average BMI and the average body circumference measurements (WC, mid-upper arm circumference and calf circumference) of males were higher than that of females, and the average skinfold thickness of females was higher than that of the males, which is consistent with the results of adult epidemiological survey in China (16). After HSCT, the anthropometric results showed that the patients have significant reduction in weight, HC, WHR, calf circumference, mid-upper arm circumference, and suprailiac skinfold thickness compared to pre-HSCT measurements. Specifically, male patients on an average lost 4 kg and female patients lost 3 kg, but these changes have no statistical significance. Male patients had 5 cm, 4 cm, and 2 cm reductions in hip, calf and mid-upper arm circumferences, respectively. Female patients had modest and statistically insignificant decreases in hip and mid-upper arm circumferences. The measurements of body circumference and skinfold thickness are simple and convenient with small error, and thus suitable for bedridden patients who cannot undergo weight measurements, or patients with excessive fluid accumulation such as hydrothorax and ascites. In addition, significant reduction (2–5 cm) of these indicators after HSCT is sensitive enough to assess the nutritional status of patients, which should be paid great attention.
This study employed combined nutritional status assessment in patients with hematological diseases, by different nutrition evaluation methods at different stages of transplantation, and indicated that: 1) Evaluation results from NRS-2002 only represent whether the patient is at risk for malnutrition, but its efficacy in estimating the grade of malnutrition is relatively weak; 2) Comparative analysis of nutritional assessment screening in post-transplantation patients using MUST revealed significantly different results from those obtained using NRS-2002; and 3) In malnutrition diagnosis among post-transplantation patients, SGA assessment indicated that 83.3% of patients have moderate to severe malnutrition, while MNA evaluated 19.27% of patients as affected by malnutrition, which is probably due to over-subjectivity of SGA, thus leading to an increase in the probability of malnutrition. Regardless of which evaluation method or single measurement indicator is used, the evidence shows that the patients with hematological diseases suffer from significantly deteriorated nutritional status after transplantation, and are at relatively high nutritional risk.
Results from this study showed that in order to perform comprehensive analysis, we need to employ different evaluation methods based on the stages of the disease in treating complex diseases such as hematological diseases, which would ensure more objective, rigorous and accurate evaluation of the nutritional status of patients. Before HSCT, some patients already had nutritional risk or nutritional deficiencies, and prompt and close nutritional screening or assessment should be performed. The nutritional status of patients after transplantation was generally deteriorated compared with that before transplantation. Body measurements should be taken more frequently during the subsequent treatment window in the laminar air flow rooms. After HSCT, it is recommended to combine MNA and SGA to evaluate the overall nutritional status of patients, and thus provide timely and reasonable nutritional treatment.
Conclusions
Appropriate nutritional support protocol originates from timely and accurate nutritional assessment. Combined nutritional evaluation methods should be used before and after HSCT. In the future, we will perform exploratory research on the nutritional support strategy for HSCT patients at different treatment stages, which may provide scientific evidence for patient-specific nutritional support and treatment strategy.
Acknowledgements
None.
Footnote
Conflicts of Interest: The authors have no conflicts of interest to declare.
References
- Huang XJ. Hematopoietic stem cell transplantation in China: current status and prospects. Am J Blood Res 2011;1:90–7. [PubMed]
- Martin-Salces M, de Paz R, Canales MA, et al. Nutritional recommendations in hematopoietic stem cell transplantation. Nutrition 2008;24:769–75. [PubMed] DOI:10.1016/j.nut.2008.02.021
- Wang B, Yan X, Cai J, et al. Nutritional assessment with different tools in leukemia patients after hematopoietic stem cell transplantation. Chin J Cancer Res 2013;25:762–9. [PubMed] DOI:10.3978/j.issn.1000-9604.2013.12.09
- Liu P, Zhang ZF, Cai JJ, et al. NRS2002 assesses nutritional status of leukemia patients undergoing hematopoietic stem cell transplantation. Chin J Cancer Res 2012;24:299–303. [PubMed] DOI:10.1007/s11670-012-0267-8
- Liu P, Yan X, Wang BS, et al. Three methods assess nutritional status of leukemia patients before hematopoietic stem cell transplantation. Chin Med J (Engl) 2012;125:440–3. [PubMed]
- Wang X, Yin T, Liu J, et al. Evaluation methods for human body nutritional status.Tianjin: Tianjin Science and Technology Press, 1982.
- Shi H, Li W, Qi Y, et al. Nutritional screening and evaluation.Beijing: People's Medical Publishing House, 2014.
- Cooperative Meta-Analysis Group of the Working Group on Obesity in China, International Life Sciences Institute, Focal Point in China. The recommendation of Chinese adult body mass index classification. Zhonghua Yu Fang Yi Xue Za Zhi (in Chinese) 2001;35:349–50.
- Vellas B, Guigoz Y, Garry PJ, et al. The mini nutritional assessment (MNA) and its use in grading the nutritional state of elderly patients. Nutrition 1999;15:116–22. [PubMed] DOI:10.1016/S0899-9007(98)00171-3
- Rullier L, Lagarde A, Bouisson J, et al. Nutritional status of community-dwelling older people with dementia: associations with individual and family caregivers' characteristics. Int J Geriatr Psychiatry 2013;28:580–8. [PubMed] DOI:10.1002/gps.v28.6
- Hanisah R, Suzana S, Lee FS. Validation of screening tools to assess appetite among geriatric patients. J Nutr Health Aging 2012;16:660–5. [PubMed] DOI:10.1007/s12603-012-0056-6
- Isenring EA, Banks M, Ferguson M, et al. Beyond malnutrition screening: appropriate methods to guide nutrition care for aged care residents. J Acad Nutr Diet 2012;112:376–81. [PubMed] DOI:10.1016/j.jada.2011.09.038
- Stratton RJ, Hackston A, Longmore D, et al. Malnutrition in hospital outpatients and inpatients: prevalence, concurrent validity and ease of use of the ‘malnutrition universal screening tool' (‘MUST') for adults. Br J Nutr 2004;92:799–808. [PubMed] DOI:10.1079/BJN20041258
- Jiang ZM, Chen W, Zhang ST. Malnutrition risk screening in 5, 303 inpatients from 11 metropolitan general hospitals and 6 specialty clinics (midterm summary abstract). Zhongguo Lin Chuang Ying Yang Za Zhi (in Chinese) 2006;14:263.
- Konturek PC, Herrmann HJ, Schink K, et al. Malnutrition in hospitals: it was, is now, and must not remain a problem!. Med Sci Monit 201;21:2969–75. [PubMed] DOI:10.12659/MSM.894238
- Zhang R, Xue C, Wang W, et al. Assessment of anthropo-metric measurements in 988 healthy adults of Han nationality. Ying Yang Xue Bao (in Chinese) 2000;22:179–82.