
Cancer incidence and mortality in China in 2013: an analysis based on urbanization level
Introduction
Cancer is one of the major non-communicable diseases in the world, including China. It has been the leading cause of death with about one fourth of all deaths in China (1). The National Central Cancer Registry (NCCR) is responsible for collecting population-based cancer registration data from local cancer registries for cancer statistics and publishing cancer registry annual report. The cancer registration data are widely used not only for cancer control and decision making, but also for scientific research (2). In this article, we provide a comprehensive overview of cancer incidence and mortality rates, as well as the new cancer cases and deaths in different urbanized areas of China in 2013.
Materials and methods
Data source
The NCCR is a department of National Cancer Center, in charge of population-based cancer registry with responsibility of data collection, evaluation and publication from local cancer registries in China. By June 1, 2016, 347 cancer registries (126 cities and 221 counties) from 31 provinces submitted data of 2013 to the NCCR. The total population covered about 287,284,044 people, accounting for about 21.11% of the national population at the end of 2013, and there were 255 qualified registries finally accepted for this analysis. All cancer cases were classified according to the International Classification of Diseases for Oncology, 3rd edition (ICD-O-3) and the International Statistical Classification of Diseases and Related Health Problems 10th Revision (ICD-10).
Quality control
All data were checked and evaluated by NCCR based on “Guideline for Chinese Cancer Registration” and referring to relevant data quality criterion of “Cancer Incidence in Five Continents Volume IX” by International Agency for Research on Cancer/International Association of Cancer Registries (IARC/IACR) (3). The data included in the final analysis should meet the following criteria: the percentage of cases morphologically verified (MV) (%) was not lower than 66%, the percentage of death certificate-only cases (DCO) (%) was lower than 15%, the mortality to incidence ratio (M/I) was between 0.6 and 0.8, and the percentage of the diagnosis of unknown basis (UB) (%) was lower than 5%.
Statistical analysis
Urbanization rate (the proportion of non-agricultural population), which obtained from the statistics of Ministry of Public Security of China (4), was used to classify all cities/counties into high, middle and low areas with the 70% and 30% as the cut-points. The cancer incidence and mortality were calculated by gender and age groups in different areas. The numbers of new cases and deaths from 255 cancer registries were reported by the top 10 cancer sites. The Chinese population in 2000 and World Segi’s population were used for age-standardized rates. The cumulative risk of developing or dying from cancer before 75 years of age (in the absence of competing causes of death) was calculated and presented as a percentage. Software including MS-Excel, IARCcrgTools2.05 issued by IARC and IACR were used for data checking and evaluation (5). All statistical analysis was conducted by SAS software (SAS Institute Inc., Cary, USA).
Results
Data quality
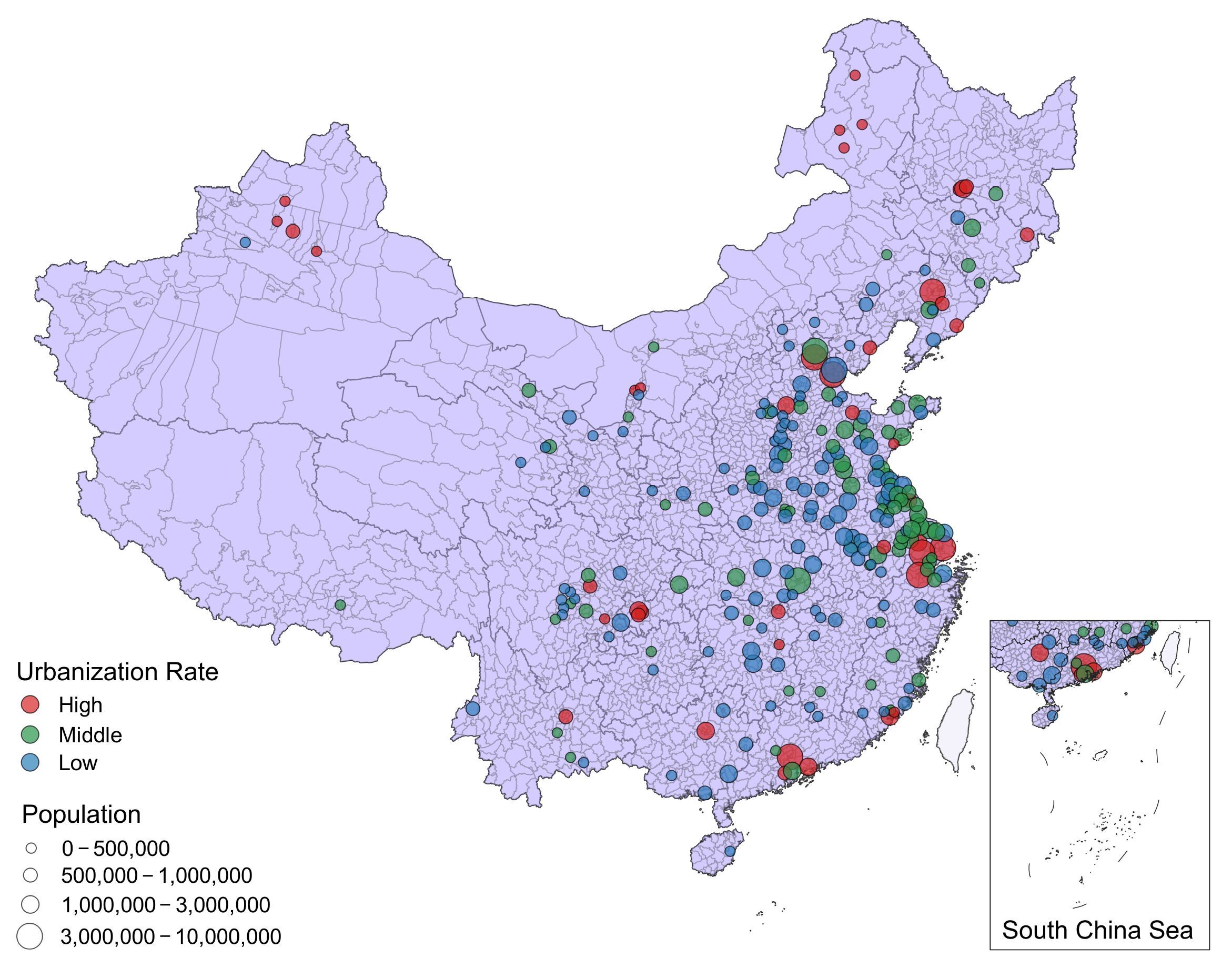
There were 255 cancer registries accepted by this analysis, distributed in 31 provinces, including 43 high urbanized ratio cities/counties, 83 middle urbanized ratio cities/counties and 129 low urbanized ratio cities/counties. The populations covered about 226,494,490 persons by 255 cancer registries, including 114,860,339 males and 111,634,151 females, accounted for 16.65% of national population in end of 2013. The geographical distribution, the covered population and urbanization levels of the 255 registries are shown in Figure 1. The overall indicators of MV%, DCO%, and M/I ratio were 68.04%, 1.74% and 0.62, respectively.
Incidence and mortality of overall cancers
Incidence
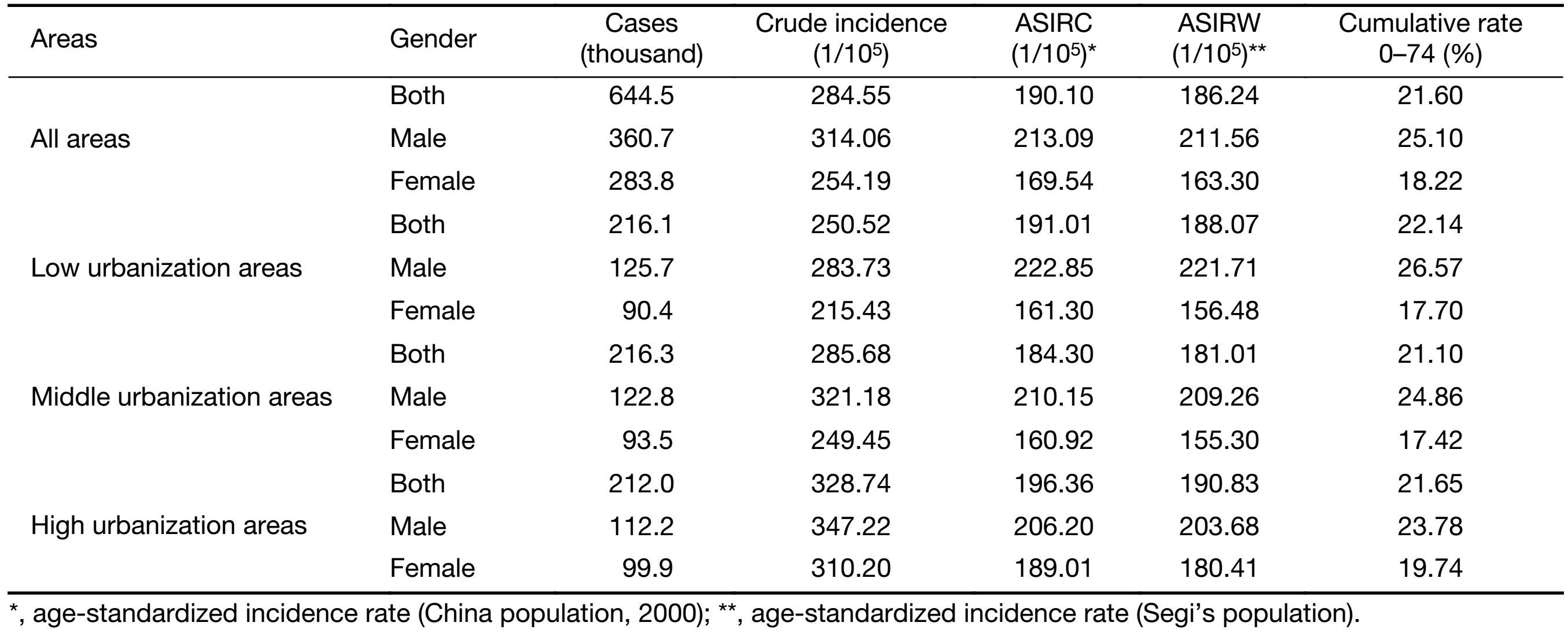
The results of cancer incidence for 255 cancer registries can be found in Table 1, and the distribution of those cancer registries in China is shown in Figure 1. Briefly, there were 644,500 new cases diagnosed as cancer from 255 cancer registries in 2013. The crude incidence rate of all cancers was 284.55/100,000 (314.06/100,000 in males and 254.19/100,000 in females). The age-standardized incidence rates by Chinese standard population (ASIRC) and by world standard population (ASIRW) were 190.10/100,000 and 186.24/100,000, respectively. Among the cancer patients aged 0−74 years, the cumulative incidence rate was 21.60%.
Full table
The high urbanization areas have a high crude incidence rate (328.74/100,000), followed by the middle and low urbanization areas. While there was a U-shaped association between age-standardized incidence rate and urbanized ratio with the middle urbanization areas having the lowest ASIRC (184.30/100,000) and ASIRW (181.01/100,000). The patterns of crude incidence rate in males and females were similar to that of all population. However, after adjusted by age, cancer incidence rate for males in low urbanization areas was higher than that in high and middle urbanization areas. But for females, cancer incidence rate was much higher in high urbanization areas than that of low and middle urbanization areas both for crude and age-adjusted incidence rate.
Mortality
The results of cancer mortality for 255 cancer registries are shown in Table 2 , and the distribution of those cancer registries in China is shown in Figure 1 .
Full table
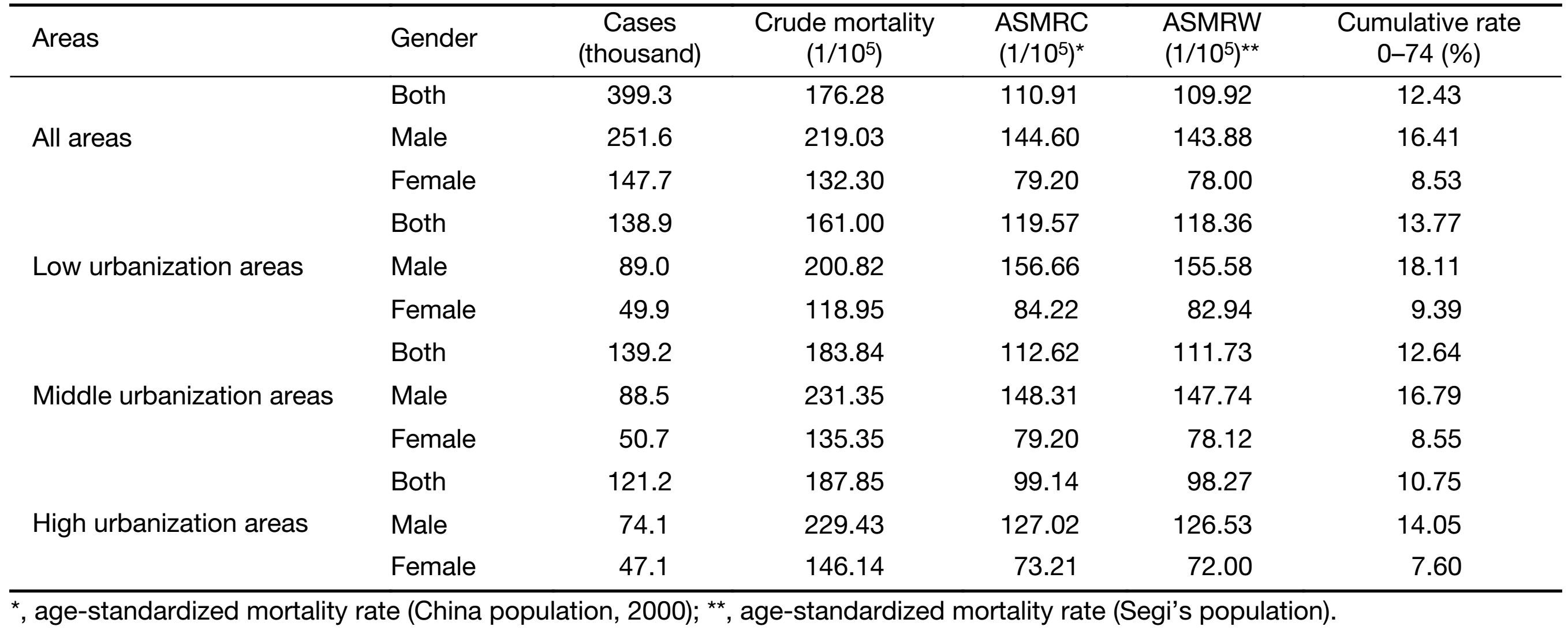
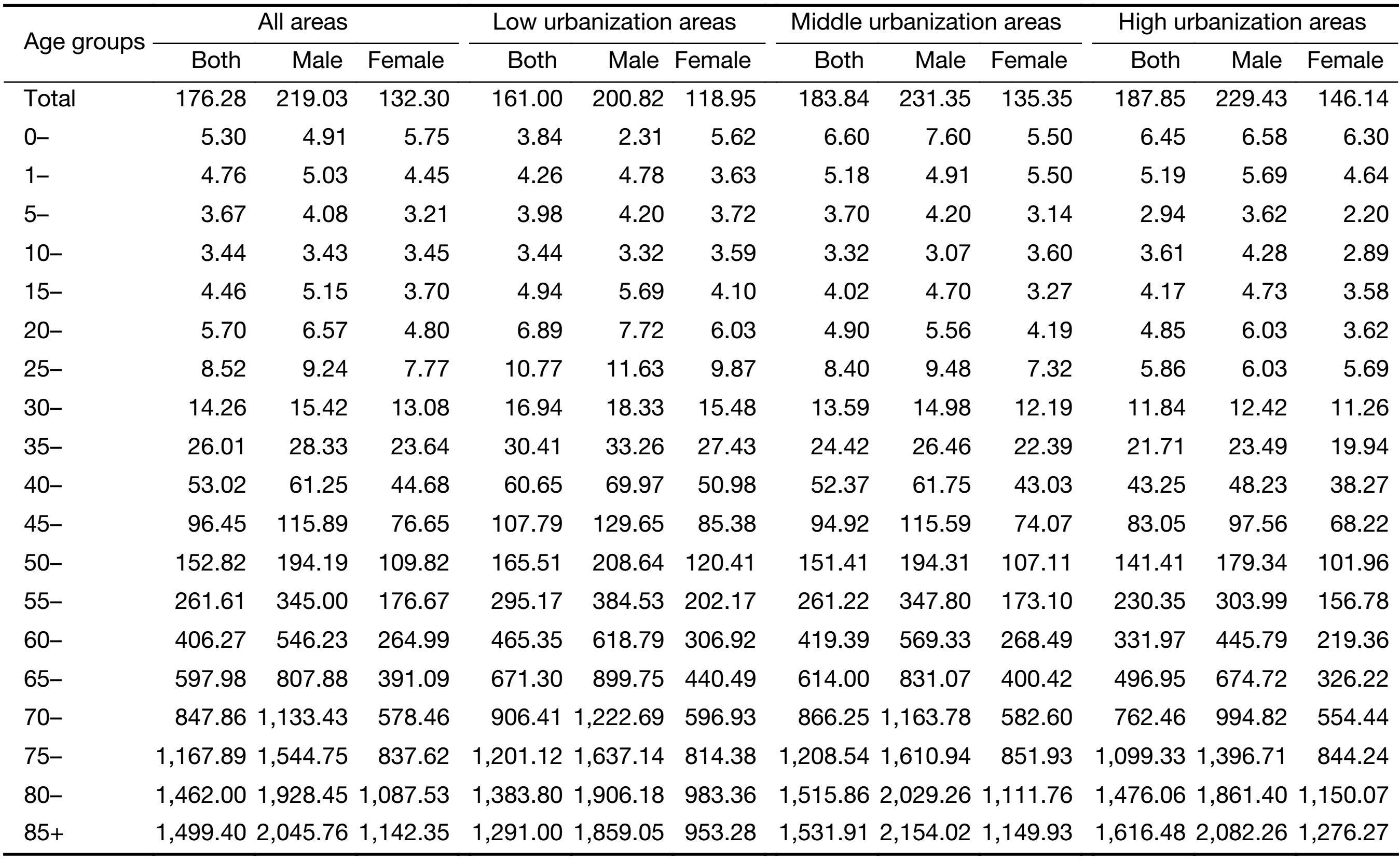
Briefly, there were 399,300 death cancer cases from 255 cancer registries in 2013. The crude mortality rate of all cancers was 176.28/100,000 (219.03/100,000 in males and 132.30/100,000 in females). The age-standardized mortality rates by Chinese standard population (ASMRC) and by world standard population (ASMRW) were 110.91/100,000 and 109.92/100,000, respectively. Among the cancer patients aged 0−74 years, the cumulative mortality rate was 12.43%.
High urbanization areas have a higher mortality rate, and middle urbanization areas came next to it followed by low urbanization areas. On the contrary, there was a negative association between age-standardized mortality rate and urbanization, with the low urbanization areas having the highest ASMRC and ASMRW but high urbanization areas having the lowest.
For males, the crude cancer mortality rate in high urbanization areas was lower than that in middle and low urbanization areas. For females, there was a negative association between age-standardized mortality rate and urbanized ratio with the high urbanization areas having the lowest crude cancer mortality rate and low urbanization areas having the highest. The patterns of ASMRC and ASMRW in males and females were similar to that of overall population.
Age-specific incidence rate
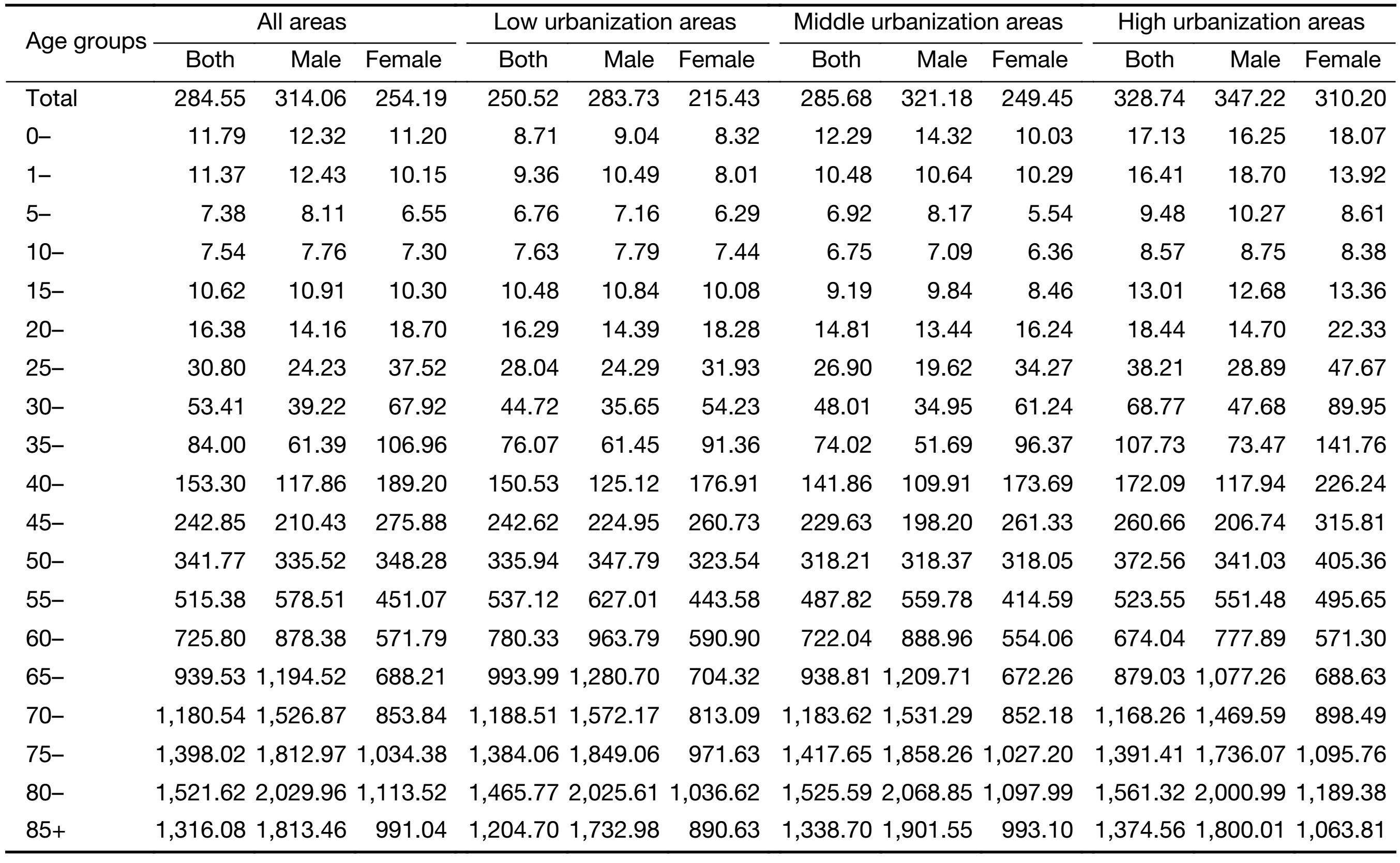
The age-specific incidence rates for 255 cancer registries are shown in Table 3. The age-specific incidence rate was relatively lower before 40 years old, while increased dramatically since then and peaked at the age group of 80−84 years. The pattern of age-specific incidence rate was similar among three urbanization areas. Between ages of 20−50 years, the age-specific incidence rate of females was higher than that of males for all areas, while the age-specific incidence rate of females was lower than that of males for all areas after age of 55 years. There was no distinct pattern for age-specific incidence rate among three urbanization areas.
Full table
Age-specific mortality rate
The age-specific mortality rates for 255 cancer registries are shown in Table 4. The age-specific mortality rate was relatively lower before 45 years and then dramatically increased, reaching peak after 85 years. The pattern of age-specific mortality rate for middle and low urbanization areas was similar to that of overall population while the age-specific mortality rate in high urbanization areas reaching peak at 80 years. For all age and all areas, the age-specific mortality rate of males was always higher than that of females. Low urbanization areas have the higher mortality rate before age of 70 years while have the lowest mortality rate after age of 80, and the same pattern can be observed in males and females.
Full table
Incidence and mortality for major cancers
Top ten leading cancer types for the new cancer cases
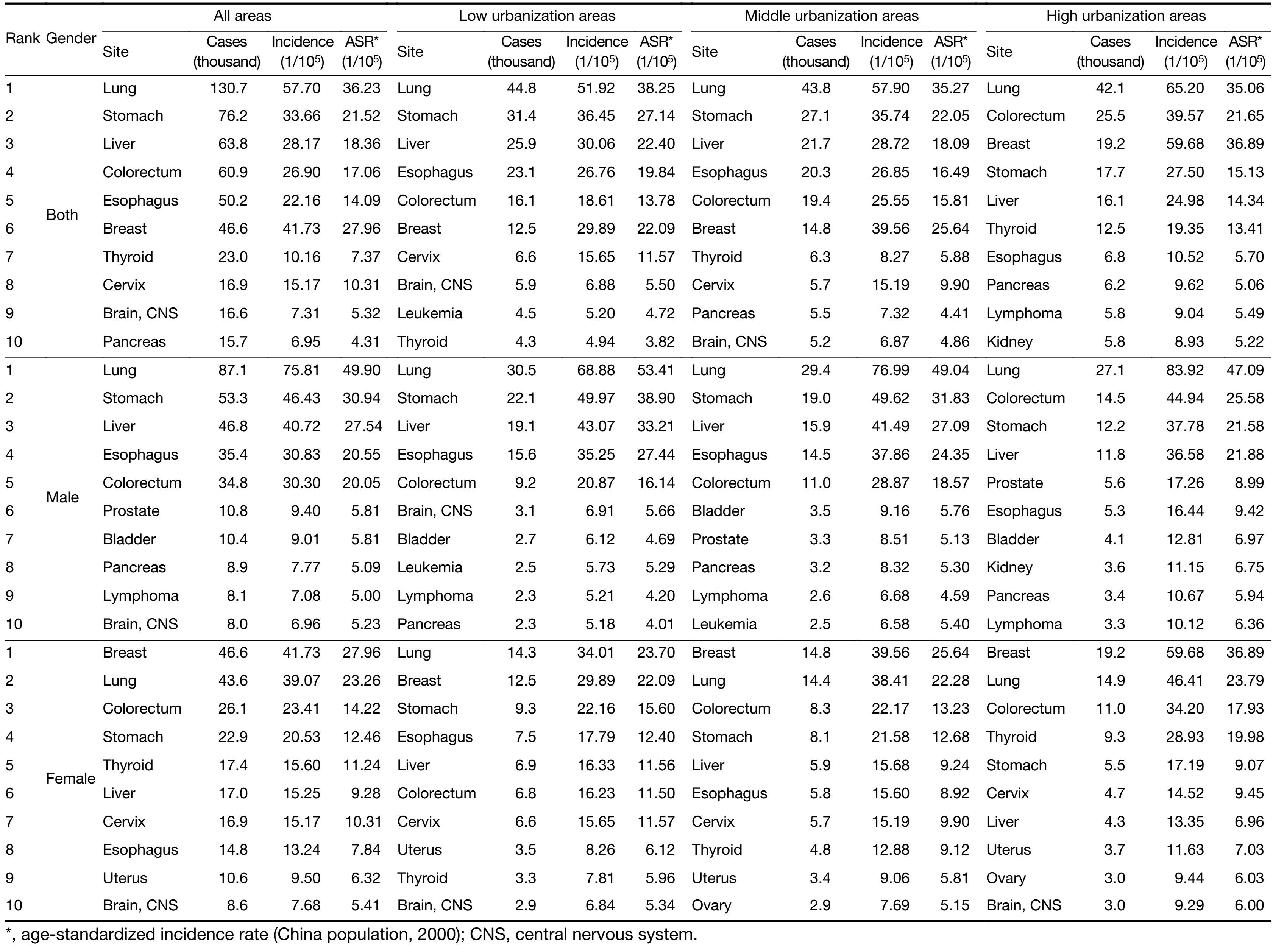
The top 10 cancer incidence rates for 255 cancer registries are shown in Table 5 . Lung cancer was the most common cancer in all areas of 255 cancer registries, followed by stomach cancer, liver cancer, colorectal cancer and esophageal cancer with new cases of 130,700, 76,200, 63,800, 60,900 and 50,200 respectively. Lung cancer was the most frequently diagnosed cancer in males followed by stomach cancer, liver cancer, esophageal cancer and colorectal cancer. Breast cancer was the most common cancer in females followed by lung cancer, colorectal cancer, stomach cancer and thyroid cancer.
Full table
In low urbanization areas, lung cancer was the most frequently diagnosed cancer, followed by stomach cancer, liver cancer, esophageal cancer and colorectal cancer with new cases of 44,800, 31,400, 25,900, 23,100 and 16,100, respectively. The most common sites of cancer were the lung, stomach, liver, esophagus and colorectum in males, while in females, cancers of the lung, breast, stomach, esophagus and liver were the most common cancers.
In middle urbanization areas, lung cancer was the most frequently diagnosed cancer, followed by stomach cancer, liver cancer, esophageal cancer and colorectal cancer with new cases of 43,800, 27,100, 21,700, 20,300 and 19,400, respectively. The most common sites of cancer were the lung, stomach, liver, esophagus and colorectum in males, while in females, cancers of the breast, lung, colorectum, stomach and liver were the most common cancers.
In high urbanization areas, lung cancer was the most frequently diagnosed cancer as well, followed by colorectal cancer, breast cancer, stomach cancer and liver cancer with new cases of 42,100, 25,500, 19,200, 17,700 and 16,100, respectively. The most common sites of cancer were the lung, colorectum, stomach, liver and prostate in males, while in females, cancers of the breast, lung, colorectum, thyroid and stomach were the most common cancers.
Top ten leading cancer types for deaths
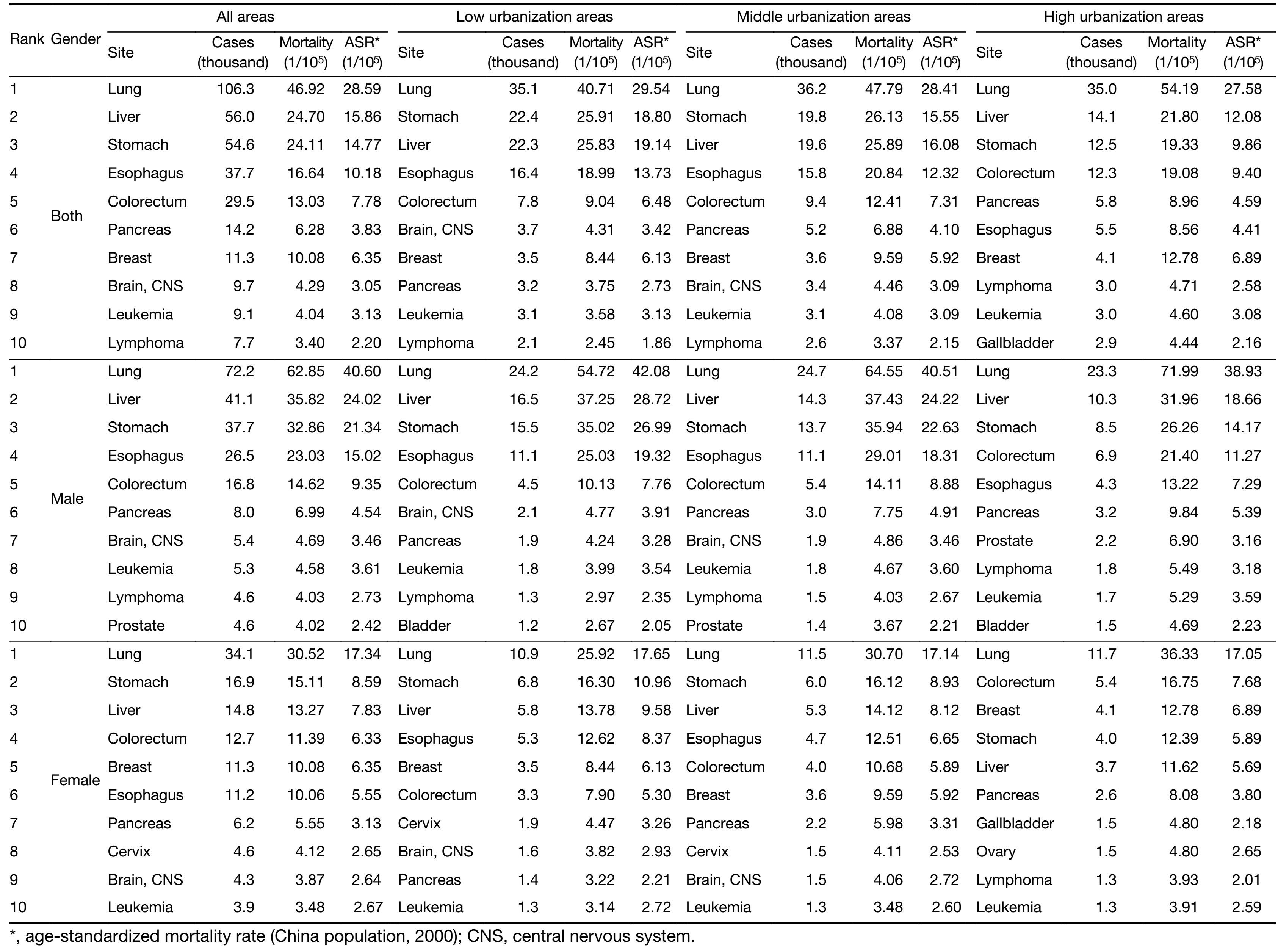
The top 10 cancer mortality rates for 255 cancer registries are shown in Table 6. Lung cancer was the leading cause of cancer death in all areas of 255 cancer registries for both males and females with the number of deaths of 72,200 and 34,100, respectively. Other cancer types with high mortality in males were liver cancer, stomach cancer, esophageal cancer and colorectal cancer. In females, stomach cancer was the second cause of cancer death, followed by liver cancer, colorectal cancer and breast cancer.
Full table
Lung cancer was the leading cause of cancer death in low urbanization areas for both males and females. The number of deaths on lung cancer in low urbanization areas was 35,100 with mortality of 40.71/100,000. The other cancer types with high mortality were liver cancer, stomach cancer, esophageal cancer and colorectal cancer in males; and stomach cancer, liver cancer, esophageal cancer and breast cancer in females.
The leading cause of cancer death in middle urbanization areas was lung cancer for both males and females. The number of deaths on lung cancer in middle urbanization areas was 36,200 with mortality of 47.79/100,000. The other cancer types with high mortality were liver cancer, stomach cancer, esophageal cancer and colorectal cancer in males; and stomach cancer, liver cancer, esophageal cancer and colorectal cancer in females.
Lung cancer was the leading cause of cancer death in high urbanization areas for both males and females as well. The number of deaths on lung cancer in high urbanization areas was 35,000 with mortality of 54.19/100,000. The other cancer types with high mortality were liver cancer, stomach cancer, colorectal cancer and esophageal cancer in males; and colorectal cancer, breast cancer, stomach cancer and liver cancer in females.
Discussion
Since 2006, NCCR of China has been publishing cancer statistics annually based on registries’ data (6-12). In these studies, the results by urban and rural areas were reported, and the difference of cancer incidence and mortality, as well as the cancer patterns between urban and rural were always being found. Therefore, we designed this study based on the latest available population-based data to explore the differences of cancer epidemiology among different urbanization areas in China.
In 2016, 347 cancer registries submitted data to the NCCR as usual, which were 86 more compared to that in 2012. The population covered about 287 millions, accounting for 21.11% of national populations. In order to ensure the quality of cancer registration data, control process was used based on the national criteria issued in program protocol. The incidence, mortality and population in the same registry have to maintain a reasonable level compared to past data. If the data are uncompleted, inexplicable or illogical, they would be sent back to the registries for check and supplement. The indicators of completeness, comparability and invalidity, such as, MV%, DCO%, MI ratio, UB% and percentage of cancer with undefined or unknown primary site (secondary) (O&U%), were used to evaluate each registry’s data to judge if submitted data are qualified or not. There were 255 registries’ data qualified for the update cancer incidence and mortality in 2013. They distributed in 31 provinces, autonomous regions and municipalities, and covered 16.65% of the national population at the end of 2013.
Compared to the data in 2012, the crude incidence and mortality rates were higher in 2013, after adjusted by age, the incidence rate was still higher, and however, the mortality rate was slightly lower than that in 2012. As a basic measure to monitor cancer information, cancer registration in China has been making a great progress in recent years (13). There were 86 more registries submitted cancer data to NCCR and 62 more qualified registries accepted for final analysis compared to 2012.
The highest crude cancer incidence and mortality rate occurred in high urbanization areas, while the low urbanization areas have the lowest crude cancer incidence and mortality. The high crude cancer incidence in high urbanization areas is mainly due to the high incidence of breast cancer and colorectal cancer, as shown in Table 5, and the crude incidence of breast and colorectal cancers in high urbanization areas is twice as higher as that in low urbanization areas. High rates of breast and colorectal cancers in high urbanization areas may be explained by health conditions and habits in these areas. As to the high crude mortality in high urbanization areas, the main causes were the high mortality of lung cancer, colorectal cancer and breast cancer in these areas. After adjusted by age, there was a U-shaped association between age-standardized incidence rate and urbanized ratio with the middle urbanization areas having the lowest ASIRC and ASIRW. Unlike with the age-standardized incidence, the sort order of age-standardized mortality among three urbanization areas was reversed completely from the crude mortality. As there was no distinct pattern for age-specific incidence rate among three urbanization areas and low urbanization areas have the lower mortality rate before age of 70 years, this reversal can be attributed to that the high urbanization areas have more older people while the low urbanization areas have more young people. All of these findings indicated that China faces the fact of high incidence of upper digestive tract cancer characterized by high incidence in developing countries; and rapid rise in lung cancer and colorectal cancer characterized by high incidence in developed countries.
Lung cancer was the leading cause of deaths in high, middle and low urbanization areas. Cigarette smoking, radon, secondhand smoke exposure and air pollution would be major factors associated with lung cancer (14,15). Household air pollution may be the main reason for lung cancer in China, especially in low urbanization areas (16). In low urbanization areas, breast cancer was much lower than that of high urbanization areas and thyroid cancer had ranked fourth, which needs to pay more attention to. Cancers from upper digestive system are still the frequent cancers in low urbanization areas, health education and promotion and early detection should be placed priority in cancer strategies. Based on the current cancer epidemiology patterns, different strategies should be implemented in different regions. Attention should be paid not only to the cancer with high incidence and mortality rates, but also to the cancer with rapid increasing trend. According to the population-based survival study in China, survival in rural areas was only half of that in urban area (17), and the main reason may be poor quality of cancer care and limited medical treatment for patients living in low urbanization areas of China (18,19). The government should balance the medical resources and take effective measures to bridge the gap.
With the economic development and changes associated with urbanization, as well as the population growth and aging, the incidence and mortality keep increasing in China. Targeted prevention, early detection and treatment programs should be carried out by health department to control the increasing cancer burden.
Acknowledgements
We acknowledged the cooperation of all the population-based cancer registries in providing cancer statistics, data collection, sorting, verification and database creation.
Funding: This study was supported by Ministry of Science and Technology of China (Grant No. 2014FY121100), and the National Natural Science Fund (Grant No. 81602931).
Footnote
Conflicts of Interest: The authors have no conflicts of interest to declare.
References
- National Bureau of Statistics of China. China Statistical Yearbook, 2010.Beijing: China Statistics Press, 2010.
- Parkin DM. The evolution of the population-based cancer registry. Nat Rev Cancer 2006;6:603–12. [PubMed] DOI:10.1038/nrc1948
- Curado MP, Edwards B, Shin HR, et al. Cancer incidence in five continents. Volume IX. IARC Sci Publ 2008:45–173. [PubMed] DOI:10.1002/ijc.25517
- Ministry of Public Security Authority. Demographic Statistics of the People’s Republic of China, 2012.Beijing: Qunzhong Press, 2014.
- Ferlay J. The IARCcrgTools Programs. Lyon: IARC, 2006. Available online: http://www.iacr.com.fr/ index.php?option=com_content&view=category&layout=blog&id=68&Itemid=445
- Chen W, Zheng R, Zuo T, et al. National cancer incidence and mortality in China, 2012. Chin J Cancer Res 2016;28:1–11. [PubMed] DOI:10.3978/j.issn.1000-9604.2016.02.08
- Chen W, Zheng R, Zeng H, et al. Annual report on status of cancer in China, 2011. Chin J Cancer Res 2015;27:2–12. [PubMed] DOI:10.3978/j.issn.1000-9604.2015.01.06
- Chen W, Zheng R, Zhang S, et al. Annual report on status of cancer in China, 2010. Chin J Cancer Res 2014;26:48–58. [PubMed] DOI:10.3978/j.issn.1000-9604.2014.01.08
- Chen W, Zheng R, Zhang S, et al. Report of incidence and mortality in China cancer registries, 2009. Chin J Cancer Res 2013;25:10–21. [PubMed] DOI:10.3978/j.issn.1000-9604.2012.12.04
- Chen WQ, Zheng RS, Zhang SW, et al. Report of incidence and mortality in China cancer registries, 2008. Chin J Cancer Res 2012;24:171–80. [PubMed] DOI:10.1007/s11670-012-0171-2
- Chen WQ, Zeng HM, Zheng RS, et al. Cancer incidence and mortality in China, 2007. Chin J Cancer Res 2012;24:1–8. [PubMed] DOI:10.1007/s11670-012-0001-6
- Chen WQ, Zhang SW, Zou XN, et al. Cancer incidence and mortality in China, 2006. Chin J Cancer Res 2011;23:3–9. [PubMed] DOI:10.1007/s11670-011-0003-9
- Wei KR, Chen WQ, Zhang SW, et al. Cancer registration in the People’s Republic of China. Asian Pac J Cancer Prev 2012;13:4209–14. [PubMed] DOI:10.7314/APJCP.2012.13.8.4209
- Ridge CA, McErlean AM, Ginsberg MS. Epidemiology of lung cancer. Semin Intervent Radiol 2013;30:93–8. [PubMed] DOI:10.1055/s-00000068
- Guo Y, Zeng H, Zheng R, et al. The association between lung cancer incidence and ambient air pollution in China: A spatiotemporal analysis. Environ Res 2016;144:60–5. [PubMed] DOI:10.1016/j.envres.2015.11.004
- Seow WJ, Hu W, Vermeulen R, et al. Household air pollution and lung cancer in China: a review of studies in Xuanwei. Chin J Cancer 2014;33:471–5. [PubMed] DOI:10.5732/cjc.014.10132
- Zeng H, Zheng R, Guo Y, et al. Cancer survival in China, 2003-2005: a population-based study. Int J Cancer 2015;136:1921–30. [PubMed] DOI:10.1002/ijc.29227
- Chen WQ, Zheng RS, Zeng HM, et al. Trend analysis and projection of cancer incidence in China between 1989 and 2008. Zhonghua Zhong Liu Za Zhi (in Chinese) 2012;34:517–24. [PubMed] DOI:10.3760/cma.j.issn.0253-3766.2012.07.010
- Zeng HM, Zheng RS, Zhang SW, et al. Trend analysis of cancer mortality in China between 1989 and 2008. Zhonghua Zhong Liu Za Zhi (in Chinese) 2012;34:525–31. [PubMed] DOI:10.3760/cma.j.issn.0253-3766.2012.07.011