
PEG-asparaginase in BFM-90 regimen improves outcomes in adults with newly diagnosed lymphoblastic lymphoma
Introduction
Lymphoblastic lymphoma (LBL) is a highly aggressive malignancy that arises from T-/B-precursor lymphoblasts. LBL is similar to acute lymphoblastic leukemia (ALL) in cellular morphology, immune phenotype, molecular genetics and clinical features. The 2008 World Health Organization (WHO) Classification classifies these two diseases as different manifestation of the same disease (1). Because cell marker expression for LBL and ALL overlaps, their clinical distinction is determined by degree of bone marrow involvement, i.e., <25% immature lymphoblasts in the bone marrow: LBL, while ≥25% immature lymphoblasts in the bone marrow: ALL (2).
LBL accounts for 2%−4% of adult non-Hodgkin lymphomas (3,4). Adult LBL has shown limited response with high relapse rates to lymphoma treatments such as the CHOP regimen (cyclophosphamide, doxorubicin, vincristine and prednisolone). Chen et al. reported a complete response (CR) rate of 17%, and median overall survival (OS) of 8.5 months (5). L-ASP-containing treatments were effective and prolonged survival of patient with ALL (6-10). However, a major limitation of L-ASP is hypersensitivity, reported in 15%−75% of both adults and children, and which in severe cases could be life-threatening and induce drug resistance (6,11,12). Also, as L-ASP has a short half-life (about 20 h), patients must be dosed every one or two days for 7 consecutive days to maintain an effective concentration of the drug (10).
To overcome these difficulties, L-ASP was covalently linked to polyethylene glycol (PEG) to formulate PEG-asparaginase (PEG-ASP). PEG-ASP preserves the enzymatic function of native L-ASP, but decreases the immunogenicity of the protein, thus potentially reducing the risk of hypersensitivity reactions. Another advantage of PEG-ASP is its prolonged half-life compared with native L-ASP; a single injection of PEG-ASP can be given instead of inconveniently administering multiple doses of native L-ASP (6,8). Comparative studies between L-ASP and PEG-ASP treatments in pediatric and adult ALL patients suggest that patients treated with PEG-ASP had faster clearance of tumor cells and more prolonged activity. Production of antibody to PEG-ASP was less than that to native L-ASP (2% vs. 26%) (11,13). The two drugs were similar in event-free survival, adverse events (AEs), and infection occurrence (11,13). PEG-ASP was approved for treatment of ALL patients allergic to L-ASP by the US Food and Drug Administration (FDA) in 1994, and has been used as first-line treatment for adult and children ALL since 2006 (14,15). However, the efficacy and safety of PEG-ASP-based pediatric regimens in adult LBL have not been well studied. In this study, we investigated the efficacy and toxicity of PEG-ASP instead of L-ASP as used in the BFM-90 regimen (PEG-ASP-BFM-90) for adult LBL.
Materials and methods
Patients
Between June 2012 and July 2015, we carried out a prospective, multicenter and single-arm clinical study, into which we recruited 30 LBL patients newly diagnosed by histomorphology and immunohistochemistry in accordance with the 2008 WHO criteria. The inclusion criteria included: 1) at least one measurable lesion; 2) aged 18−70 years, either gender; 3) Eastern Cooperative Oncology Group (ECOG) performance status score 0−3, and 4) expected survival of at least 3 months. The exclusion criteria included: 1) coagulation disorder; 2) serious failure of liver and kidney function; 3) concurrent malignant serious or uncontrolled cardiovascular diseases within the previous 6 months; 4) severe infection; 5) HIV infection; or 6) women who were lactating, pregnant, or of child-bearing potential and not using a reliable method of contraception during the study period.
All patients were required to have documentation of LBL by tumor tissue sampling of involved sites. Some patients with ≥25% bone marrow immature lymphoblasts in subsequent bone marrow examination were still classified as LBL with bone marrow involvement (stage IV), and included in the study.
Acute pancreatitis was defined in this study as any two of the following situations: 1) abdominal pain (acute onset of a persistent, severe, epigastric pain often radiating to the back); 2) serum lipase or amylase activity at least 3 times greater than the upper limit of normal; and 3) characteristic findings of acute pancreatitis on computed tomography (CT) or magnetic resonance imaging (MRI) (16). Pancreatitis was graded according to the US National Cancer Institute Common Terminology Criteria for Adverse Events (NCI CTCAE), version 4.0.
Treatment with study drug may be discontinued for any of the following reasons: 1) patient does not meet inclusion criteria; 2) protocol violation; 3) disease progression; 4) serious AEs that cannot be recovered; 5) study terminated by investigators; 6) withdrawal by subject.
Patients provided written informed consent after being informed of the nature of the disease, its treatment options, and its possible outcomes. This study was approved by the Research Ethics Committee of Peking University Cancer Hospital and carried out in accordance with the approved guidelines.
Chemotherapy
We used PEG-ASP in lieu of the native L-ASP during induction and intensification therapy for adult LBL using the BFM-90 regimen (PEG-ASP-BFM-90). Induction phase 1a: prednisone 60 mg/m2 orally on d 1 to d 28; vincristine 1.4 mg/m2 (max 2 mg) intravenously (IV) on d 1, 8, 15 and 22; daunorubicin 30 mg/m2 IV on d 1, 8, 15 and 22; PEG-ASP 2,500 IU/m2 intramuscularly (IM) on d 2 and 16, which was not capped at 3,750 IU. This cycle of treatment was repeated once. Induction phase 1b: cyclophosphamide 1,000 mg/m2 IV on d 1 and 15; cytarabine 75 mg/m2 IV on d 3 to d 6, and 17 to 20; 6-mercaptopurine 60 mg/m2 orally on d 1 to d 28. Consolidation phase: methotrexate 3,000 mg/m2 IV on d 1 and 15; 6-mercaptopurine 25 mg/m2 orally on d 1 to d 28. Reinduction phase 2a is the same as induction phase 1a. Reinduction phase 2b is the same as induction phase 1b. Maintenance phase: methotrexate 20 mg/m2 orally, once a week for 18 months; 6-mercaptopurine 60 mg/m2 orally, daily for 18 months. All patients received regular intrathecal cytarabine chemotherapy for prophylaxis central nervous system (CNS) lymphoma without prophylactic cranial radiotherapy. Local irradiation was also omitted in this study. The protocols included induction, consolidation, reinduction and maintenance; the total treatment course took two years. If the patient achieved a CR or partial response (PR), and agreed to receive high-dose chemotherapy plus autologous peripheral blood stem cell transplantation (APBSCT), it was given after the end of treatment. After APBSCT, the patient would continue with maintenance therapy.
Response and follow-up criteria
Pretreatment evaluations included history, physical examination, complete hematological and biochemical tests, CT scans of neck, chest, abdomen and pelvic, or 18F-fluorodeoxyglucose positron emission tomography if possible, cerebrospinal fluid examination, bone marrow aspirate and biopsy. Clinical staging was performed according to the Ann Arbor classification. Response was evaluated at the end of each phase of the protocol according to Cheson criteria (17). Initial responses included CR, PR, stable disease and progressive disease. OS was defined as the time from diagnosis to death from any cause, or the date of last follow-up. Progression-free survival (PFS) was measured from diagnosis to first progression, relapse after response, or death from any cause, or the date of last follow-up. AEs were graded according to the US NCI CTCAE, version 4.0.
Statistical analysis
Data were analyzed using IBM SPSS Statistics (Version 19.0; IBM Corp., New York, USA). Correlations between clinicopathological factors and CR were evaluated using a chi-squared (χ2) test or Fisher's exact test. Multifactor logistic regression was performed to adjust possible confounding factors and calculate odds ratios. Kaplan-Meier survival analysis was used to evaluate patient prognosis; P values were calculated by log-rank tests. Patients' 1-, 2- and 3-year survival rates were obtained with the life-table method. P<0.05 was considered statistically significant.
Results
Patient characteristics
We enrolled 30 patients from 5 participating institutions from China (Peking University Cancer Hospital, Peking University First Hospital, Peking University Third Hospital, Air Force General Hospital of Chinese People's Liberation Army, and the 309th Hospital of Chinese People's Liberation Army), which included 19 males and 11 females with a median age of 30 (range: 18−62) years. Immunophenotyping showed that 29 (96.7%) had T-cell disease, of whom 20 (66.7%) had mediastinal involvement, which was associated with pleural or pericardial effusions in 9 patients (30.0%). Marrow infiltration >25% was identified in 18 patients (60.0%). According to the Ann Arbor staging system, 5 patients (16.7%) had stage I-II disease, and 25 patients (83.3%) had stage III-IV disease. B symptoms were observed in 11 patients (36.7%). International prognostic index (IPI) score was ≤1 in 12 patients (40.0%). No patients showed evidence of CNS involvement at diagnosis. All patients (100%) underwent chemotherapy, and all patients completed 128 times of PEG-ASP, with the median of 4 (range: 2−6) times. No patients combined their treatment with radiotherapy. Their clinical characteristics at diagnosis are summarized inTable 1.
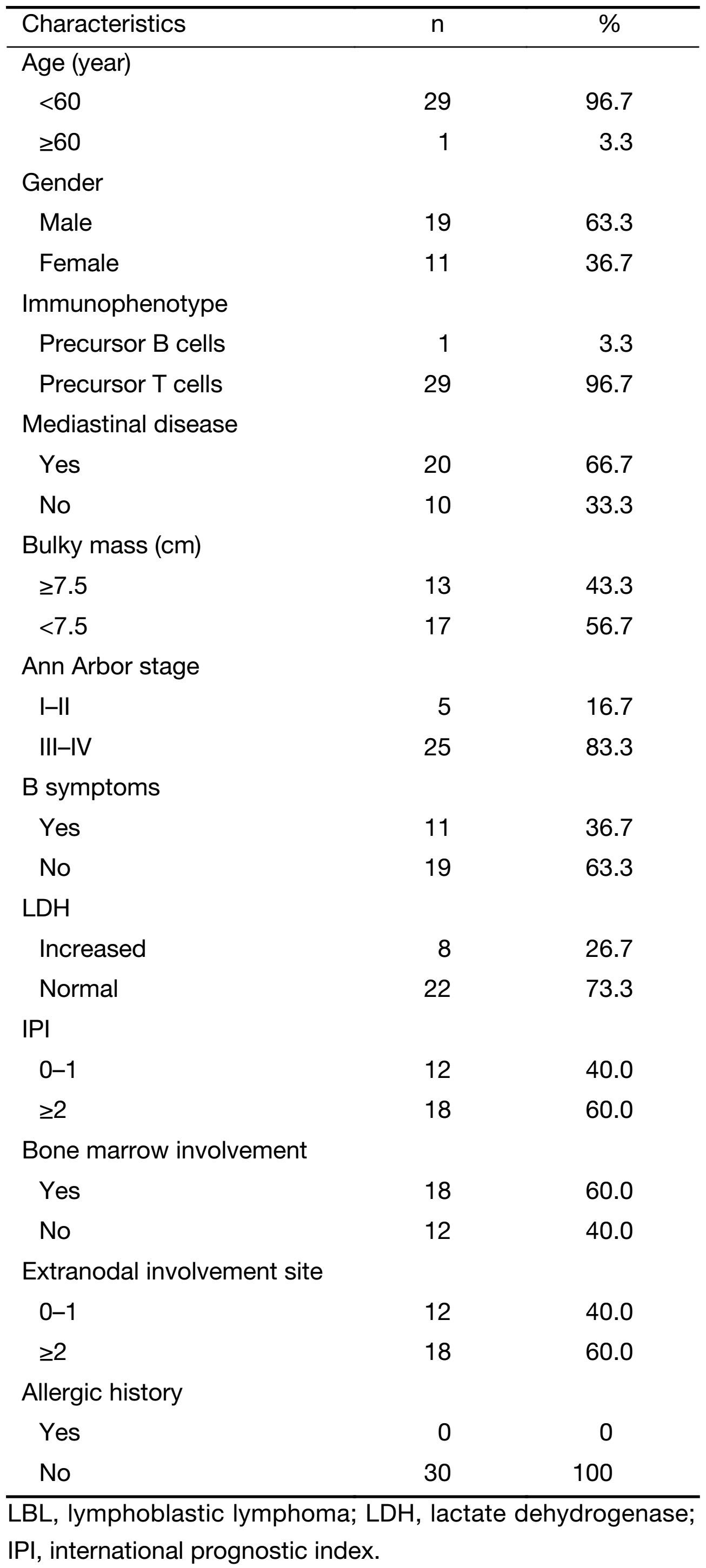
Full table
Response
Response rates at the end of treatment were overall response rate (ORR) 86.7% (26/30); CR 50.0% (15/30); and PR 36.7% (11/30). We found treatment had low efficacy for patients with bulky masses (≥7.5 cm; P<0.05). Patients with mediastinal disease at diagnosis had poorer responses; their CR rate was only 35%, compared with an 80% CR rate for those without mediastinal disease (P=0.05). However, other clinical factors, including age, gender, cell origin, stage, lymphoma B symptoms, lactate dehydrogenase levels, IPI score, bone marrow involvement and extranodal involvement, did not affect chemotherapy outcomes (Table 2).
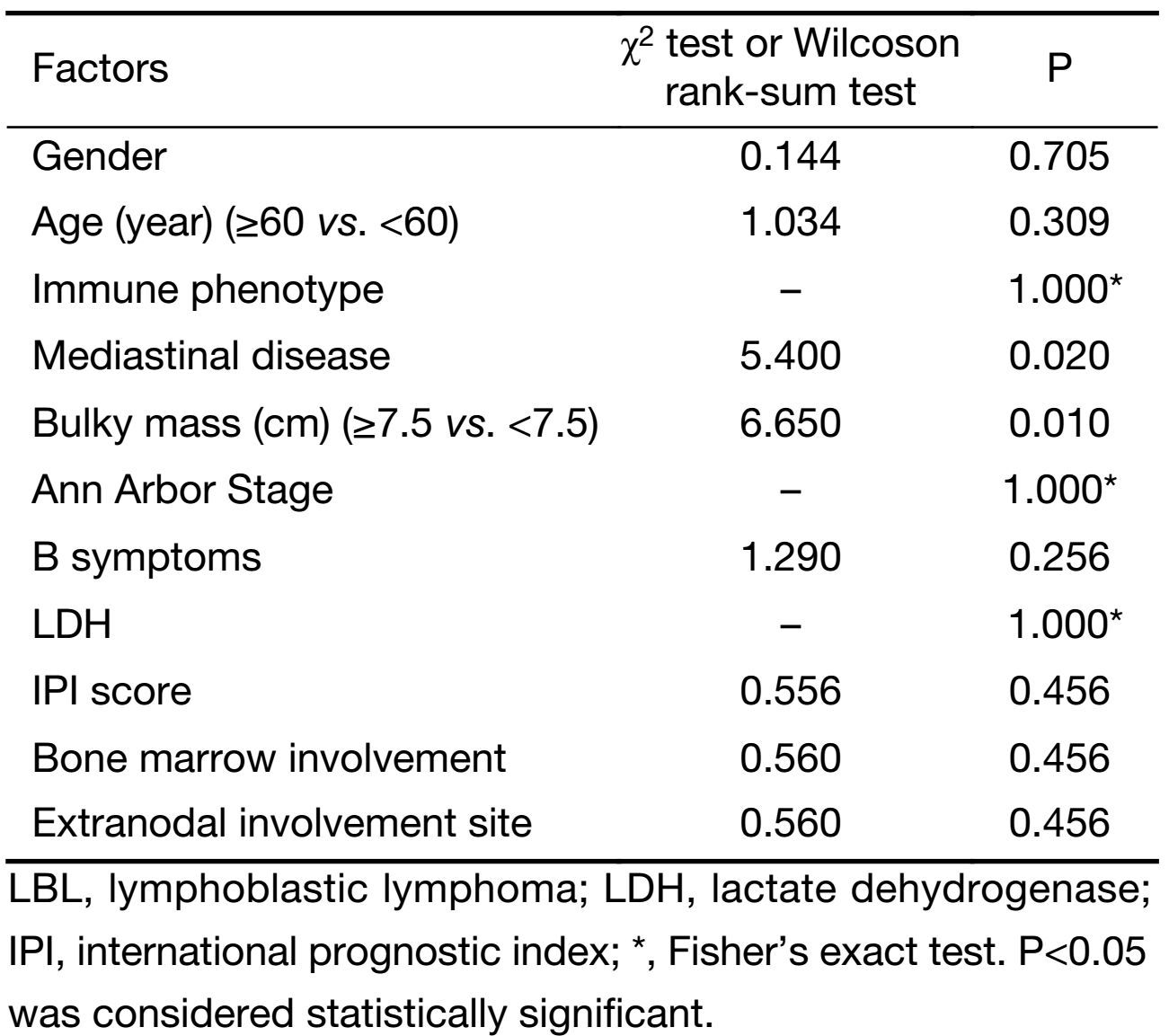
Full table
Follow-up and survival
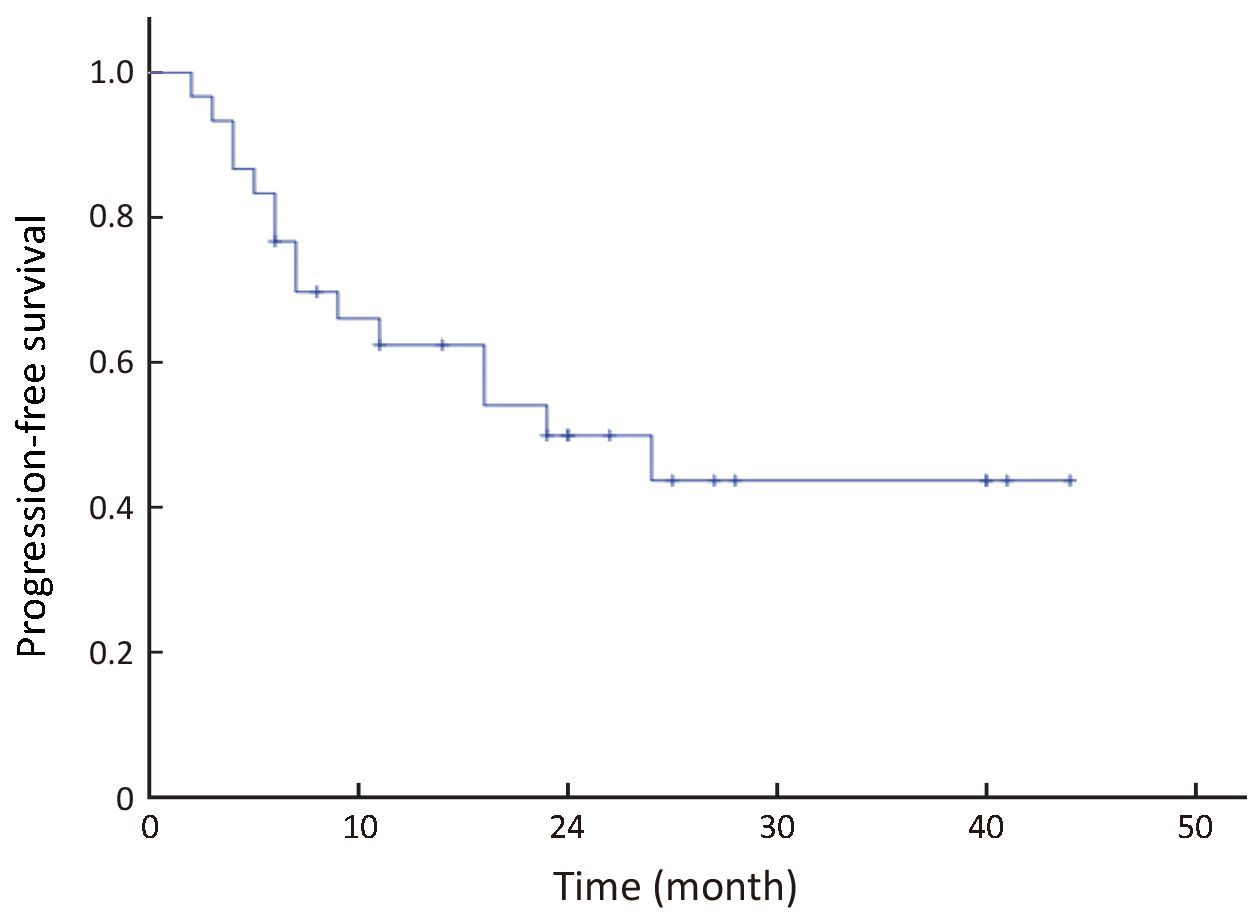
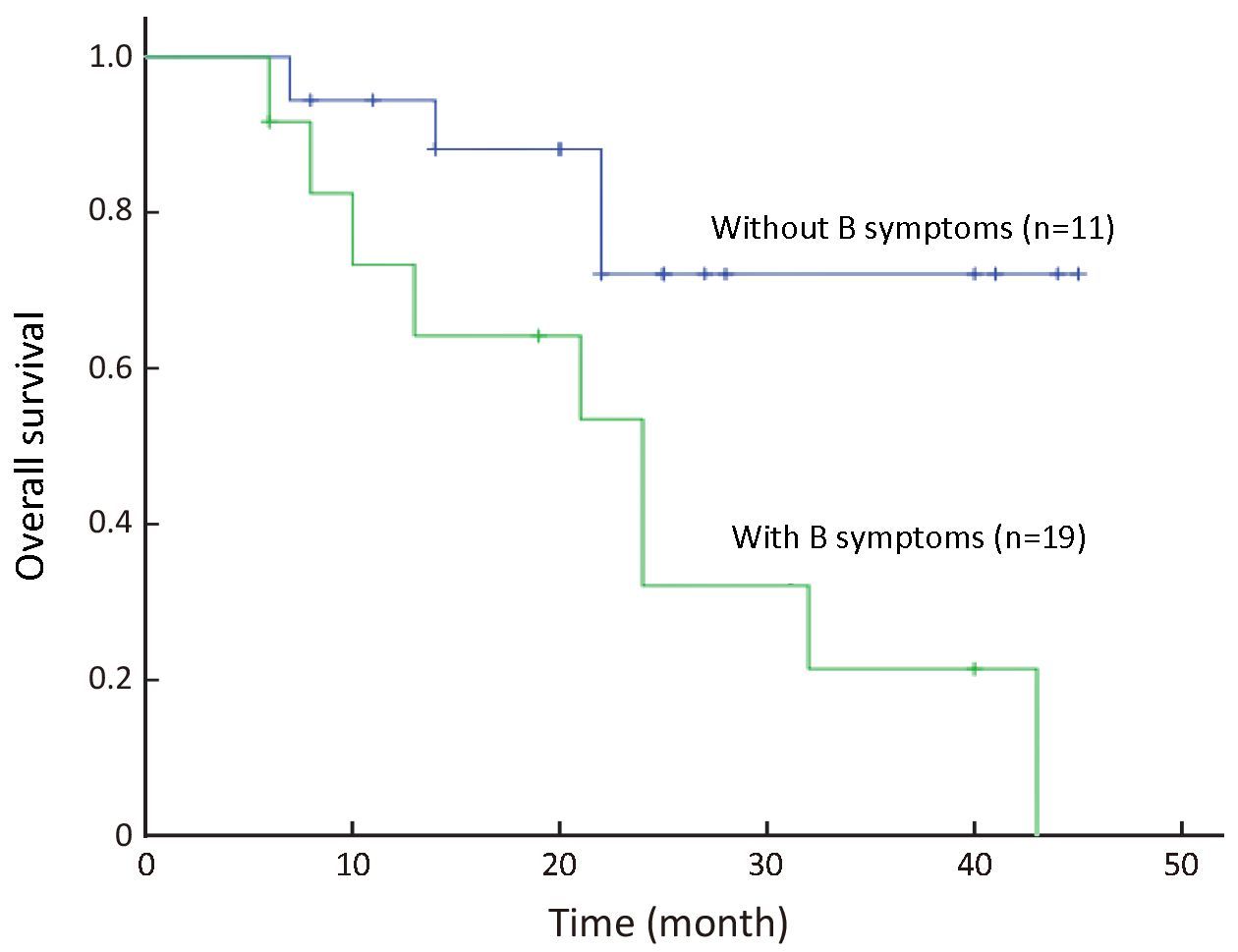
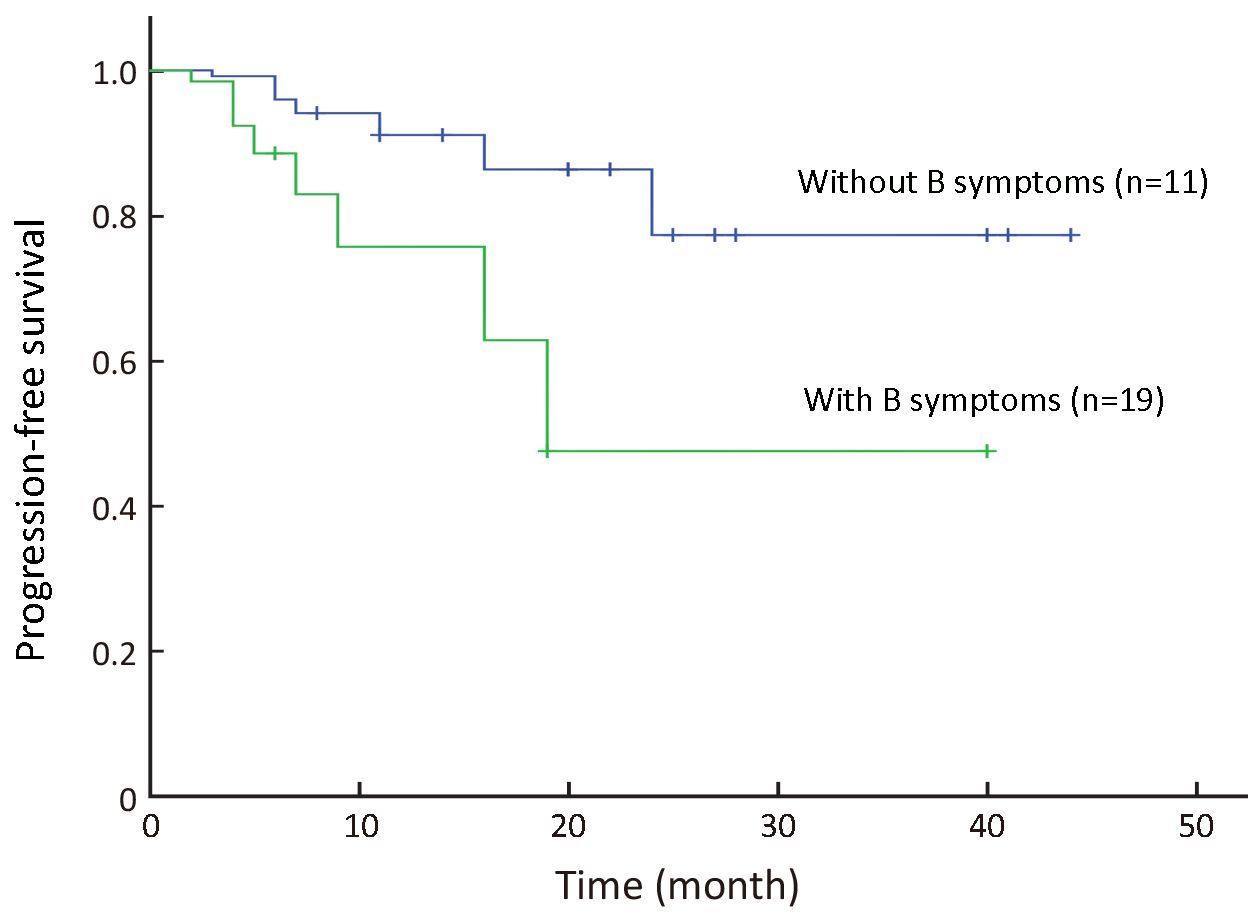
All 30 patients were eligible for survival analysis. The median follow-up period for all patients was 22 (range: 6−45) months. Since treatment, 13 patients have died of tumor relapse and progression. The estimated median OS is 30 months. The 3-year OS was 46.0% [95% confidence interval (95% CI), 28.2%−64.8%; Figure 1]; and 3-year PFS was 43.0% (95% CI, 25.7%−62.0%; Figure 2). In univariate comparison with patients who did not have lymphoma B-symptoms at diagnosis, the 3-year OS was significantly less for patients with B symptoms at diagnosis (23.5% vs. 67.2%, P=0.048; Figure 3), although the 3-year PFS did not significantly differ from patients with B symptoms (19.38% vs. 55.91%, P=0.090; Figure 4). The CR patients had significantly better 3-year PFS than those with inferior responses (63.64% vs. 19.26%, P=0.036), but they did not significantly differ in 3-year OS (51.13% vs. 31.89%, P=0.485). Other clinical factors (age, gender, cell origin, stage, lactate dehydrogenase levels, IPI score, bone marrow involvement, bulky mass, mediastinal disease and extranodal involvement) did not affect prognosis.

No patients received allogeneic hematopoietic stem cell transplantation. However, two female patients, aged 20 and 32 years old, with stage IV disease, received APBSCT after achieving CR from the PEG-ASP-BFM-90 regimen. They are both still alive.
Adverse effects
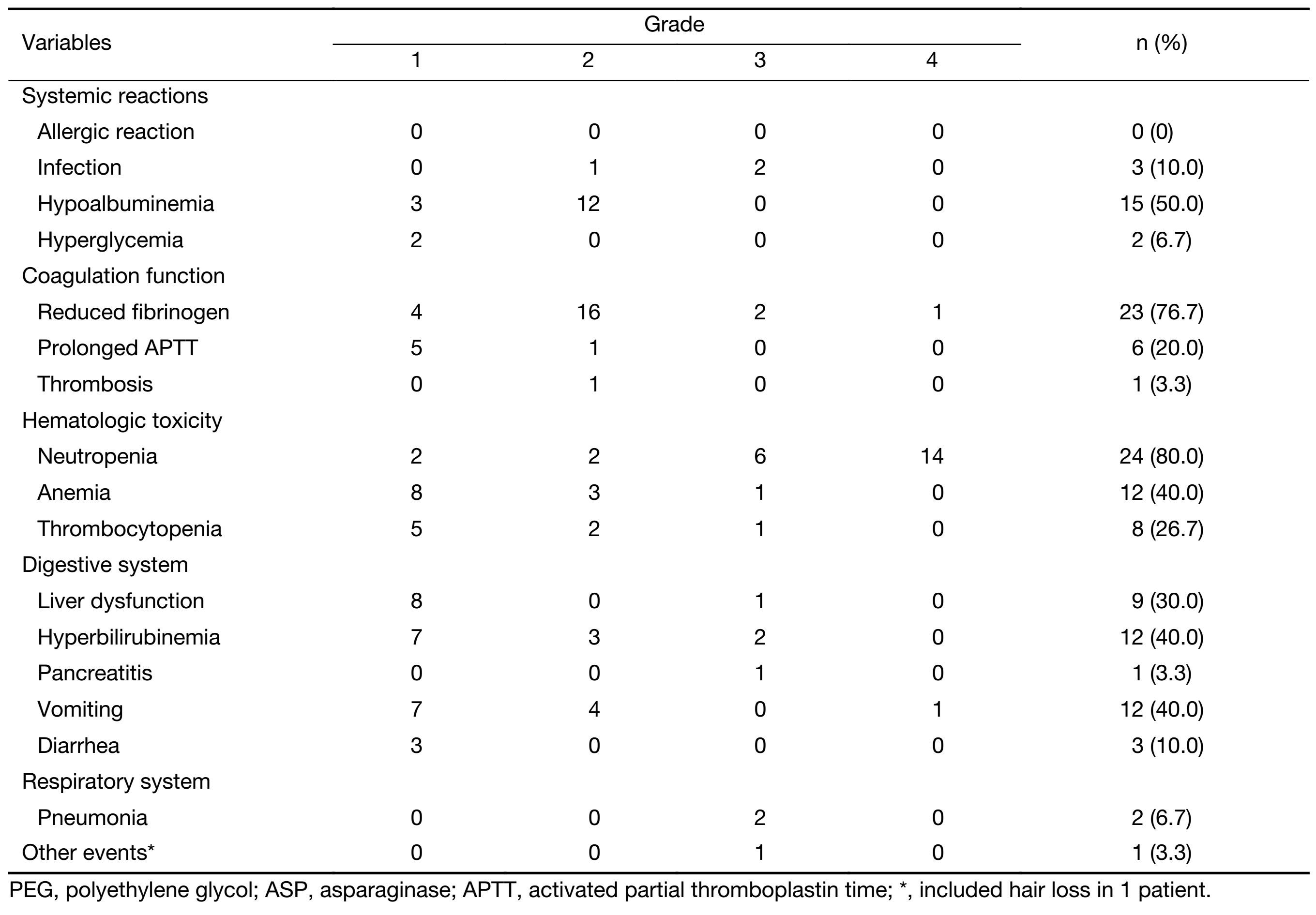
Although we observed AEs in all 30 patients (Table 3), we saw no therapy-related deaths or allergic reactions that occurred during treatment. Most AEs were grade 1−2. We found many patients had bone marrow suppression (80.0%), and 66.6% had grade 3−4 neutropenia. Twelve patients (40.0%) had anemia (including 1 with grade 3−4 anemia); 8 (26.7%) had thrombocytopenia (1 with grade 3−4), and 20 (66.7%) had grade 1−2 fibrinogen reduction (but without other clinical occurrence of mucocutaneous or visceral hemorrhage); 15 (50.0%) had hypoalbuminemia (none with grade 3−4).
Full table
We assayed plasma D-dimer levels in 8 patients, 7 of which had elevated levels during PEG-ASP-BFM-90 treatment, and 1 had a lower level. Three patients developed infections (recovered after stopping treatment), including 2 with pulmonary infections (who completed the full treatment) and 1 patient with septicemia (who withdrew from further treatment). One patient with pancreatitis discontinued PEG-ASP-containing treatment. Other common AEs included liver dysfunction and digestive tract toxicities (Table 3).
Discussion
L-ASP is an enzyme of bacterial origin that hydrolyzes serum asparagine to aspartate and ammonia. Serum asparagine depletion results in inhibited protein synthesis and subsequent tumor cell death, whereas normal cells can synthesize asparagine (10). However, hypersensitivity reactions to L-ASP limit its application. PEG-ASP has lower immunogenicity and been a standard treatment for pediatric ALL. In this study, we investigated the efficacy and toxicity of PEG-ASP substituted for L-ASP in the BFM-90 regimen for adult LBL.
Patients in our study were younger, with males about twice as many as females. Most patients had grossly enlarged mediastinums, which manifested as cough, shortness of breath, dyspnea, and/or superior vena cava syndrome. Their clinical characteristics were similar to those in previous studies (18,19). When immunophenotyped, 96.7% had T-lineage disease; only 1 patient had B-lineage disease.
PEG-ASP dosing studies have been performed for both pediatric and adult patients with ALL. In general, a single intravenous dose of PEG-ASP at 2,500 IU/m2 replaced the 9−14 injections of native L-ASP used in the original BFM protocol (6,13). In our study, 30 patients received PEG-ASP [2,500 IU/m2 intramuscular injection (single maximum dose 3,750 IU)] on d 2 and d 16 of the 4-drug induction course. Our result showed that the 2,500 IU/m2 dose is safe for in adult LBL patients when PEG-ASP was integrated into a pediatric regimen (19). Intramuscular injection is more convenient and comfortable than intravenous injection. Of the 30 patients, 37% received all 6 doses of PEG-ASP; 70% received 4 doses. Only 17% of patients needed to discontinue the treatment because of serious toxicity (20).
Results of the PEG-ASP-BFM-90 regimen for adult LBL were encouraging. The ORR was 86.7% (26/30) with 50.0% (15/30) CR, 46% 3-year OS, and 43% 3-year PFS, but with lower efficacy in patients with bulky masses (P<0.05), and significantly lower 3-year OS for those with B symptoms. These results compare favorably with studies of a CHOP-like regimen, in which the CR rate was only 17% and median OS was 8.5 months (5). Wetzler et al. reported 83% ORR with PEG-ASP-containing regimen in adult ALL (12). Chang et al. showed 83.6% ORR with L-ASP-containing therapeutic regimens among 46 adult LBL (21). These results are similar to those of our study. Shi et al. suggested consolidation with stem cell transplantation during first complete remission for chemosensitive adult LBL (22). Two of our patients received APBSCT after effective treatment and are still alive.
CNS involvement at presentation occurs in 20% of cases and is a frequent site of relapse without CNS prophylaxis. In PEG-ASP-BFM-90 scheme, CNS prophylaxis is based on corticosteroids, intrathecal cytarabine, and intravenous high-dose methotrexate infusion without cranial irradiation (23). None of the patients developed CNS lymphoma. This suggests that the combination of high-dose methotrexate and intrathecal chemotherapy (usually 10 intrathecal injections in our study) was adequate CNS protection.
Most AEs in our study cohort were grade 1−2, with no therapy-related deaths. The most common AEs were neutropenia, anemia and thrombocytopenia, and were similar to those seen in BFM-90 with L-ASP (14,24,25). We also observed grade 1−2 fibrinogen reduction in 20 patients (66.7%), but no increase in hemorrhage occurred. In this study, chemotherapy was stopped when the plasma fibrinogen was <150 mg/dL; patients underwent infusions of fresh plasma or fibrinogen when plasma fibrinogen level was <100 mg/dL (26). One patient had thrombus at the venous catheter site which improved after anticoagulation treatment. Albayrak et al. found elevated plasma D-dimer levels during treatments that contained L-ASP (27); similarly, we observed elevated D-dimer levels during PEG-ASP-containing treatment. We speculate that PEG-ASP has an effect on hemorrhage and coagulation balance (28). Hypoalbuminemia is also a common AE. Ping et al. found that 8 of 32 lymphoma patients on PEG-ASP-based chemotherapy had hypoalbuminemia (29); whereas 15 (50.0%) of our patients developed grade 1−2 hypoalbuminemia. In our study, the pancreatitis occurrence was lower. The result was very similar to previous reports, including studies that used PEG-ASP and native L-ASP (6,13). Douer et al. reported that incidences of grade 3−4 hyperbilirubinemia and transaminitis were 31% and 63%, respectively (20). Aldoss et al. showed that grade 3−4 hyperbilirubinemia and transaminitis occurred in 23.7% and 53.9% of patients, respectively (30). Our results showed that grade 3−4 hyperbilirubinemia (6.7%) and transaminitis (3.3%) were lower than those reported for adults. This may be related to the low fat diets during treatment.
Hypersensitivity to PEG-ASP was clearly less than that to L-ASP, for which reported hypersensitivity reaction rates were 15%−75% (11,12). We saw no occurrence of clinical allergic reactions among our 30 patients during all 128 times of PEG-ASP. Our patients each received a dose of dexamethasone (10 mg IV) before each starting PEG-ASP. This may reduce the frequency of clinical hypersensitivity (13). Kurtzberg et al. reported that even patients who were allergic to L-ASP could still use PEG-ASP (31).
Efficacy of PEG-ASP-or L-ASP-containing BFM-90 regimens for LBL or ALL is better for children than adults. The most common AEs in children were bacteremia infectious (13,29), whereas the most common AEs in adults were neutropenia. Incidence and type of other AEs were similar in both age groups (13,32).
Conclusions
Our clinical data and observed outcomes indicate that 1 dose of PEG-ASP can replace multiple doses of native L-ASP in BFM-90, with predominantly grade 3−4 neutropenia for adults LBL and no therapy-related deaths. Efficacy was similar to that in previous reports of PEG-ASP-containing regimens for adult ALL, but was lower for patients with bulky masses; patients with lymphoma B symptoms also had poorer survival outcomes. Major advantages include less serious allergic reactions, 2−3 weeks of action duration, and convenience for patients and physicians. These initial results provide new data and more evidence for Chinese patients from the 5 study sites in China. However, further studies are required to assess the benefits of PEG-ASP-BFM-90.
Acknowledgements
We thank Dr. Xinqiang Ji from Peking University Cancer Hospital & Institute for statistical analysis support. We also thank various research units for their meticulous data collection.
Footnote
Conflicts of Interest: The authors have no conflicts of interest to declare.
References
- Swerdlow SH, Campo E, Harris NL, et al. WHO Classification of Tumours of Haematopoietic and Lymphoid Tissues. 4th edition.Lyon: IARC Press, 2008.
- Murphy SB. Classification, staging and end results of treatment of childhood non-Hodgkin's lymphomas: dissimilarities from lymphomas in adults. Semin Oncol 1980;7:332–9. [PubMed]
- Thomas DA, O'Brien S, Cortes J, et al. Outcome with the hyper-CVAD regimens in lymphoblastic lymphoma. Blood 2004;15;104:1624–30. [PubMed] DOI:10.1182/blood-2003-12-4428
- Sun J, Yang Q, Lu Z, et al. Distribution of lymphoid neoplasms in China: analysis of 4,638 cases according to the World Health Organization classification. Am J Clin Pathol 2012;138:429–34. [PubMed] DOI:10.1309/AJCP7YLTQPUSDQ5C
- Chen YC, Ho CL, Kao WY, et al. Adult lymphoblastic lymphoma in Taiwan: an analysis of treatment results of 26 patients. Ann Hematol 2001;80:647–52. [PubMed] DOI:10.1007/s002770100363
- Douer D, Yampolsky H, Cohen LJ, et al. Pharmacodynamics and safety of intravenous pegaspargase during remission induction in adults aged 55 years or younger with newly diagnosed acute lymphoblastic leukemia. Blood 2007;109:2744–50. [PubMed] DOI:10.1182/blood-2006-07-035006
- Kawedia JD, Rytting ME. Asparaginase in acute lymphoblastic leukemia. Clin Lymphoma Myeloma Leuk 2014;14:S14–7. [PubMed] DOI:10.1016/j.clml.2014.06.017
- Kumar K, Kaur J, Walia S, et al. L-asparaginase: an effective agent in the treatment of acute lymphoblastic leukemia. Leuk Lymphoma 2014;55:256–62. [PubMed] DOI:10.3109/10428194.2013.803224
- Curran E, Stock W. How I treat acute lymphoblastic leukemia in older adolescents and young adults. Blood 2015;125:3702–10. [PubMed] DOI:10.1182/blood-2014-11-551481
- Moscardó Guilleme C, Fernández Delgado R, Sevilla Navarro J, et al. Update on L-asparaginase treatment in paediatrics. An Pediatr (Barc) (in Spanish) 2013;79:329.e1–329.e11. [PubMed] DOI:10.1016/j.anpedi.2013.03.015
- Panetta JC, Gajjar A, Hijiya N, et al. Comparison of native E. coli and PEG asparaginase pharmacokinetics and pharmacodynamics in pediatric acute lymphoblastic leukemia. Clin Pharmacol Ther 2009;86:651–8. [PubMed] DOI:10.1038/clpt.2009.162
- Wetzler M, Sanford BL, Kurtzberg J, et al. Effective asparagine depletion with pegylated asparaginase results in improved outcomes in adult acute lymphoblastic leukemia: Cancer and Leukemia Group B Study 9511. Blood 2007;109:4164–7. [PubMed] DOI:10.1182/blood-2006-09-045351
- Avramis VI, Sencer S, Periclou AP, et al. A randomized comparison of native Escherichia coli asparaginase and polyethylene glycol conjugated asparaginase for treatment of children with newly diagnosed standard-risk acute lymphoblastic leukemia: a Children's Cancer Group study. Blood 2002;99:1986–94. [PubMed] DOI:10.1182/blood.V99.6.1986
- Dinndorf PA, Gootenberg J, Cohen MH, et al. FDA drug approval summary: pegaspargase (oncaspar) for the first-line treatment of children with acute lymphoblastic leukemia (ALL). Oncologist 2007;12:991–8. [PubMed] DOI:10.1634/theoncologist.12-8-991
- Alvarnas JC, Brown PA, Aoun P, et al. Acute lymphoblastic leukemia, Version 2.2015. J Natl Compr Canc Netw 2015;13:1240–79. [PubMed]
- Greenberg JA, Hsu J, Bawazeer M, et al. Clinical practice guideline: management of acute pancreatitis. Can J Surg 2016;59:128–40. [PubMed] DOI:10.1503/cjs
- Cheson BD, Pfistner B, Juweid ME, et al. Revised response criteria for malignant lymphoma. J Clin Oncol 2007;25:579–86. [PubMed] DOI:10.1200/JCO.2006.09.2403
- Bassan R, Maino E, Cortelazzo S. Lymphoblastic lymphoma: an updated review on biology, diagnosis and treatment. Eur J Haematol 2016;96:447–60. [PubMed] DOI:10.1111/ejh.2016.96.issue-5
- Vinogradova IuE, Chernova NG, Kaplanskaia IB, et al. Long-term results of treatment for T-cell lymphoblastic lymphomas. Ter Arkh (in Russian) 2012;84:57–60. [PubMed]
- Douer D, Aldoss I, Lunning MA, et al. Pharmacokinetics-based integration of multiple doses of intravenous pegaspargase in pediatric regimen for adults with newly diagnosed acute lymphoblastic leukemia. J Clin Oncol 2014;32:905–11. [PubMed] DOI:10.1200/JCO.2013.50.2708
- Chang MH, Kim SJ, Kim K, et al. Clinical features and treatment outcomes of adult B-and T-lymphoblastic lymphoma: results of multicentre analysis in Korea. Leuk Lymphoma 2009;50:1119–25. [PubMed] DOI:10.1080/10428190902926999
- Shi Y, Zhou S, He X, et al. Autologous hematopoietic stem cell transplantation in chemotherapy-sensitive lymphoblastic lymphoma: treatment outcome and prognostic factor analysis. Chin J Cancer Res 2015;27:66–73. [PubMed] DOI:10.3978/j.issn.1000-9604.2015.02.04
- Burkhardt B, Woessmann W, Zimmermann M, et al. Impact of cranial radiotherapy on central nervous system prophylaxis in children and adolescents with central nervous system-negative stage III or IV lymphoblastic lymphoma. J Clin Oncol 2006;24:491–9. [PubMed] DOI:10.1200/JCO.2005.02.2707
- Stock W, Douer D, DeAngelo DJ, et al. Prevention and management of asparaginase/pegasparaginase-associated toxicities in adults and older adolescents: recommendations of an expert panel. Leuk Lymphoma 2011;52:2237–53. [PubMed] DOI:10.3109/10428194.2011.596963
- Earl M. Incidence and management of asparaginase-associated adverse events in patients with acute lymphoblastic leukemia. Clin Adv Hematol Oncol 2009;7:600–6. [PubMed]
- Ogawa C, Manabe A, Ohara A, et al. Current national and international status of supportive therapy for the coagulopathy associated with L-asparaginase containing regimen for acute lymphoblastic leukemia. Rinsho Ketsueki (in Japanese) 2013;54:316–8. [PubMed]
- Albayrak M, Gürsel T, Kaya Z, et al. Alterations in procoagulant, anticoagulant, and fibrinolytic systems before and after start of induction chemotherapy in children with acute lymphoblastic leukemia. Clin Appl Thromb Hemost 2013;19:644–51. [PubMed] DOI:10.1177/1076029612450771
- Truelove E, Fielding AK, Hunt BJ. The coagulopathy and thrombotic risk associated with L-asparaginase treatment in adults with acute lymphoblastic leukaemia. Leukemia 2013;27:553–9. [PubMed] DOI:10.1038/leu.2012.290
- Ping LY, Zheng W, Wang XP, et al. Safety and adverse event profiling of pegylated L-asparaginase combined chemotherapy in the treatment of lymphoma. Zhonghua Yi Xue Za Zhi (in Chinese) 2012;92:3257–60. [PubMed]
- Aldoss I, Douer D, Behrendt CE, et al. Toxicity profile of repeated doses of PEG-asparaginase incorporated into a pediatric-type regimen for adult acute lymphoblastic leukemia. Eur J Haematol 2016;96:375–80. [PubMed] DOI:10.1111/ejh.2016.96.issue-4
- Kurtzberg J, Asselin B, Bernstein M, et al. Polyethylene Glycol-conjugated L-asparaginase versus native L-asparaginase in combination with standard agents for children with acute lymphoblastic leukemia in second bone marrow relapse: a Children's Oncology Group Study (POG 8866). J Pediatr Hematol Oncol 2011;33:610–6. [PubMed] DOI:10.1097/MPH.0b013e31822d4d4e
- Cooperation Group of Phase II Clinical Trial of PEG-Asp. Comparison of polyethylene glycol conjugated asparaginase and L-asparaginase for treatment of childhood acute lymphoblastic leukemia. Zhonghua Xue Ye Xue Za Zhi (in Chinese) 2008;29:29–33. [PubMed]