
A national report from China Liver Transplant Registry: steroid avoidance after liver transplantation for hepatocellular carcinoma
Introduction
Hepatocellular carcinoma (HCC), which has high incidence and mortality rates in China (1), is a malignant disease with limited therapeutic options due to its aggressive progression (2,3). Liver transplantation (LT) is the only curative alternative for selected patients with HCC who are not eligible for resection and/or with decompensated cirrhosis. In China, donor livers are often offered to HCC patients who have hepatitis B virus (HBV)-related backgrounds. Unfortunately, HCC recurrence has been reportedly as high as 40% after LT, and tumor recurrence remains the main cause of death of HCC patients after LT (4,5). Tumor progression is more rapid and aggressive in immunosuppressed patients following LT. Steroids play a crucial role in rejection prophylaxis and treatment after LT and other solid organ transplantation. Since the first LT was performed by Thomas Starzl in 1963, steroids have been very popular as immunosuppressive (IS) drugs, together with calcineurin inhibitors (CNIs), resulting in a decrease in acute rejection (AR) in recent decades, but their usage has become more controversial recently. Increasing attention has been focused on the side effects associated with steroid-based IS regimens (6). Long-term steroids can facilitate the host immunity, which maybe the cause of HCC recurrence (7-10). In addition, the numerous side effects of steroids, such as infections, obesity, lipid profile imbalances, hypertension and diabetes mellitus, have emphasized the need to avoid or limit steroid usage (11,12).
In the past decade, that avoidance or withdrawal of steroids after LT could decrease the risks of various side effects has been confirmed in Western patients with hepatitis C virus (HCV) infections but rarely in Chinese HBV patients, particularly HBV-related HCC patients (13-18). It is therefore essential to assess the effectiveness and safety of steroid-free IS regimens in Chinese patients. In this large-sample retrospective research, we were particularly interested in the impact of this steroid-free regimen on the incidence of HBV-related HCC recurrence after LT, because these patients account for nearly half of the Chinese liver transplant population, and recurrence of the disease is such a significant problem in this patient population.
Materials and methods
Study population
The details of 20,829 liver transplants, performed from January 2000 to December 2011, were collected by the China Liver Transplant Registry (CLTR) from 76 liver transplantation centers across China.
A total of 18,362 patients were excluded from this study using the following exclusion criteria: LT for non-tumor lesions or non-HBV disease; LT for other malignant tumors (cholangiocarcinoma, carcinoma of gallbladder, mixed carcinoma, and secondary tumors); patients exceeding the Hangzhou criteria (19); pediatric LT; steroids administered pre-transplantation; re-transplantation or combined liver-kidney transplantation; incomplete laboratory and clinical data; or death within 1 week due to bleeding after LT.
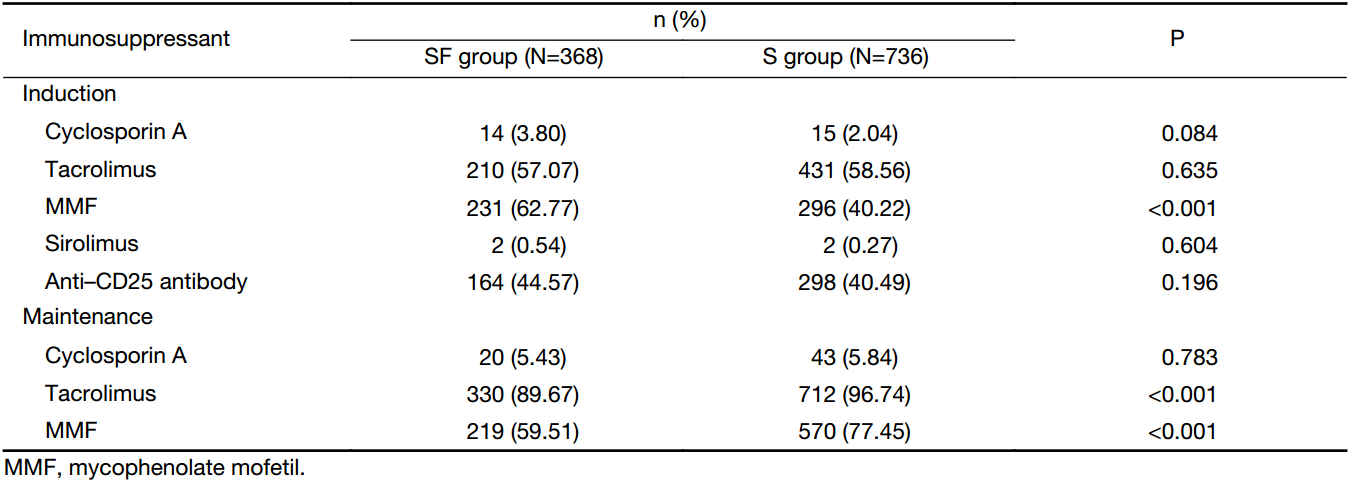
The remaining 2,467 patients were enrolled, and their data were used for analysis. Three hundred sixty-eight patients received corticosteroid-free immunosuppression (SF group). The steroid-free IS regimen consisted of a CNI [either tacrolimus (FK-506) or microemulsified cyclosporine A (CsA)], mycophenolate mofetil (MMF), and anti-CD25 antibody (basiliximab). In the SF group, corticosteroid was used once during the operation and then was completely avoided postoperatively, unless the patient developed AR.
The steroid-free patients were matched at a 1:2 ratio, by age, sex, donor source, hepatic encephalopathy, hepato-renal syndrome, diabetes mellitus, hypertension, model for end-stage liver disease (MELD), α-fetoprotein (AFP) level, TNM tumor staging for HCC, size of the largest tumor, number of tumor nodules and operation date with control patients receiving steroid-based immunosuppression during the same period (S group, n=736). This retrospective cohort study was performed using multivariate matched sampling methods that incorporated the propensity score (20). All the liver transplant candidates would receive ultrasound (US) and serum biochemistry test every week, computed tomography (CT) or magnetic resonance imaging (MRI) test every 4 weeks to monitor the dynamic changes of tumors. All of these patients received preoperative antiviral treatments, including monotherapy of nucleoside analogs (lamivudine or entecavir) and multiple therapies of nucleoside analogs (lamivudine plus adefovir). All patients received lamivudine (100 mg/d orally) combined with low-dose Hepatitis B immune globulin (HBIG) (2,000 IU of HBIG in the anhepatic phase, followed by 800 IU daily for the next 6 days and weekly for 3 weeks, and then 800 IU monthly thereafter ) therapy after LT (21). The steroid IS regimen used in the S group consisted of a CNI and steroid with or without MMF, depending on the need, and/or anti-CD25 antibody. In this group, methylprednisolone or prednisolone was administered at a dose of 1,000 mg intraoperatively and 100 mg on d 1, and it was tapered completely by the end of three months after LT. AR was treated by bolus steroid administration. MMF was administered as needed at the same initial dose and tapering protocol as the steroid-free IS regimen. Upon leaving the hospital, the patient receives a schedule of follow-up clinic visits for laboratory tests and checkups. The idea is to track clinical progress and to detect potential complications as early as possible. Patients are instructed to notify the transplantation team if they have any prolonged illness, fever, nausea, vomiting, or diarrhea or if they experience any unusual symptoms or adverse effects potentially related to the immunosuppressant.
Each organ donation and transplantation was strictly followed the current regulation of the Chinese Government and the Declaration of Helsinki 2004, and informed consents were obtained from all patients. The study was approved by Ethics Committee of the First Affiliated Hospital, College of Medicine, Zhejiang University.
Data collection
The following variables were recorded: age, sex, primary liver disease, body mass index (BMI), blood pressure, cold ischemia time and IS agents. The pre-transplant data were collected within 24 h before LT.
HBV recurrence was defined as the recurrence of serum HBV surface antigens. AR was identified by liver biopsy (22). AR episodes were generally treated with the administration of 500 mg of methylprednisolone daily for 3 consecutive days and 240 mg tapered to zero within the first 1 month. Hypertension was defined as blood pressure greater than 140/90 mmHg (1 mmHg=0.133 kPa) at two consecutive visits and/or the need for antihypertensive therapy.
Hyperlipidemia was defined as serum cholesterol ≥200 mg/dL (5.17 mmol/L) or the need for pharmacologic treatment 2 months after LT, and hyperlipidemia was defined as serum triglycerides ≥150 mg/dL (1.69 mmol/L) or the need for pharmacologic treatment 2 months after LT (23).
New-onset diabetes mellitus (NODM) was defined as a fasting glucose level of at least 7 mmol/L (126 mg/dL) or a non-fasting glucose level of at least 11.1 mmol/L (200 mg/dL) confirmed on at least 2 occasions or the need for anti-diabetic drugs persisting beyond the first month but within the first year after transplantation (24).
Statistical analysis
Quantitative variables are expressed as medians and ranges. Categorical variables are presented as values and percentages. The medians and ranges of continuous data were compared using the Wilcoxon rank sum test, and the Chi-square test or Fisher’s exact test was used to compare categorical variables. A multivariate logistic regression model, using clinically relevant variables, was generated to compute a propensity score for each patient. The propensity score was then used to obtain a 1:2 match for all of the enrolled patients. To identify risk factors related to tumor recurrence in steroid avoidance recipients, a multivariate analysis was performed using the logistic regression model with backward elimination. Overall survival (OS) and tumor-free survival (TFS) analysis were performed by Kaplan-Meier methodology with log rank testing. Cox proportional hazard models were used to estimate hazard ratios for OS and TFS, and to determine independent risk factors. SAS software (Version 9.2; SAS Institute Inc., Cary, NC, USA) was used to complete all of the analyses, and P<0.05 was considered statistically significant (two-tailed test).
Results
Patient characteristics
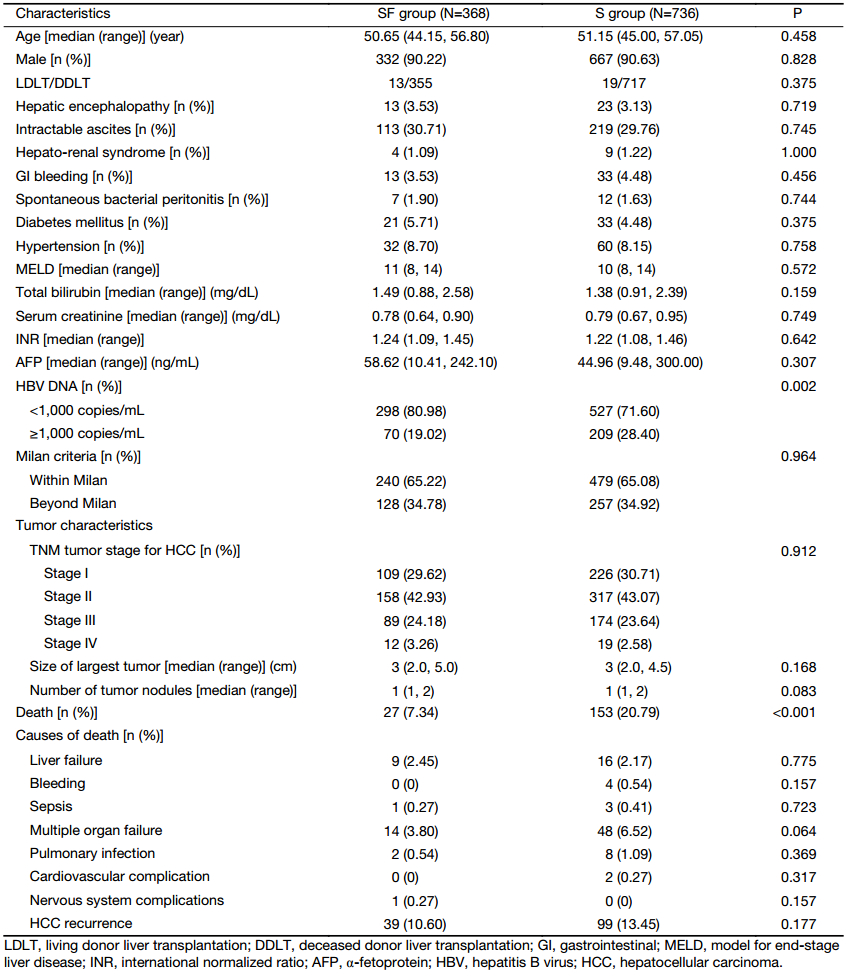
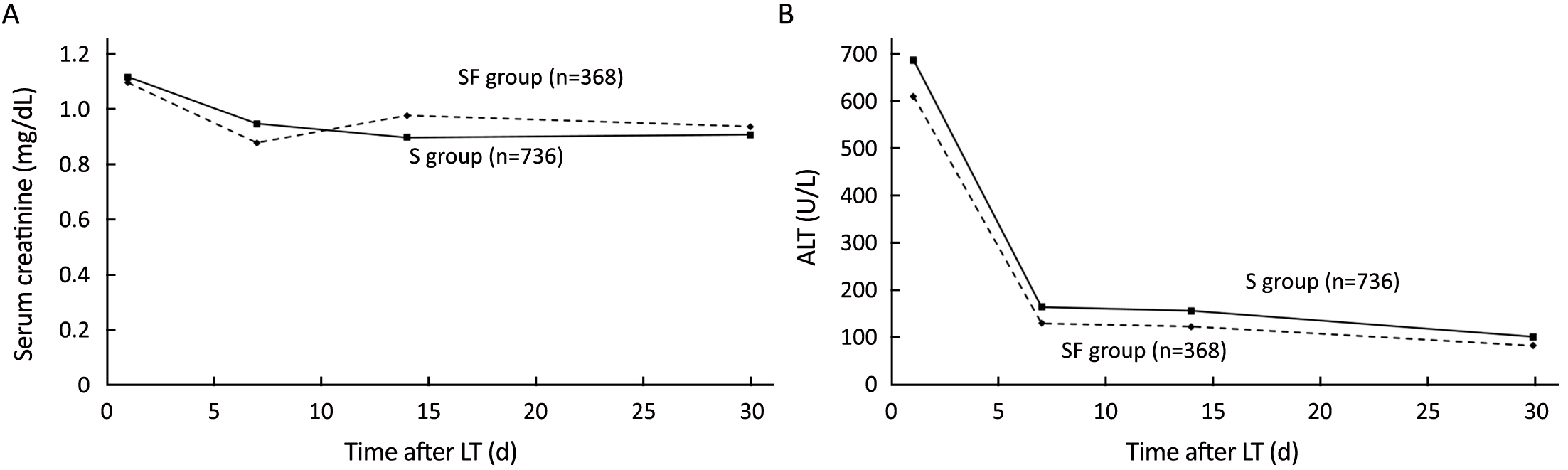
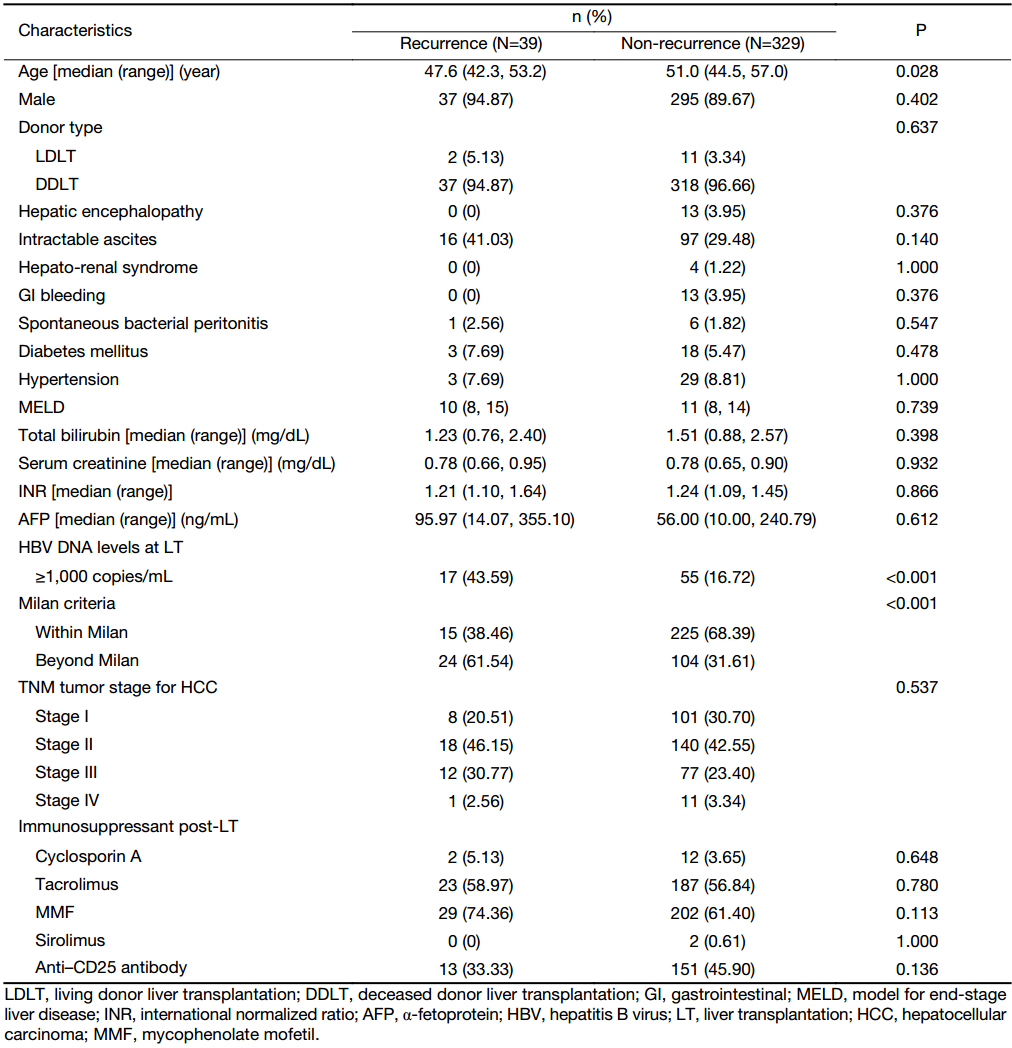
The patients’ demographic characteristics were similar between the two groups (Table 1). The follow-up periods were similar: 25.13 (range: 0.03–142.27) months in the SF group and 26.71 (range: 0.16–134.90) months in the S group (P=0.371). The serum creatinine and alanine transaminase (ALT) levels after LT (1 d, 7 d, 14 d and 30 d) were similar between the two groups (Figure 1).
Full table
Incidence of AR
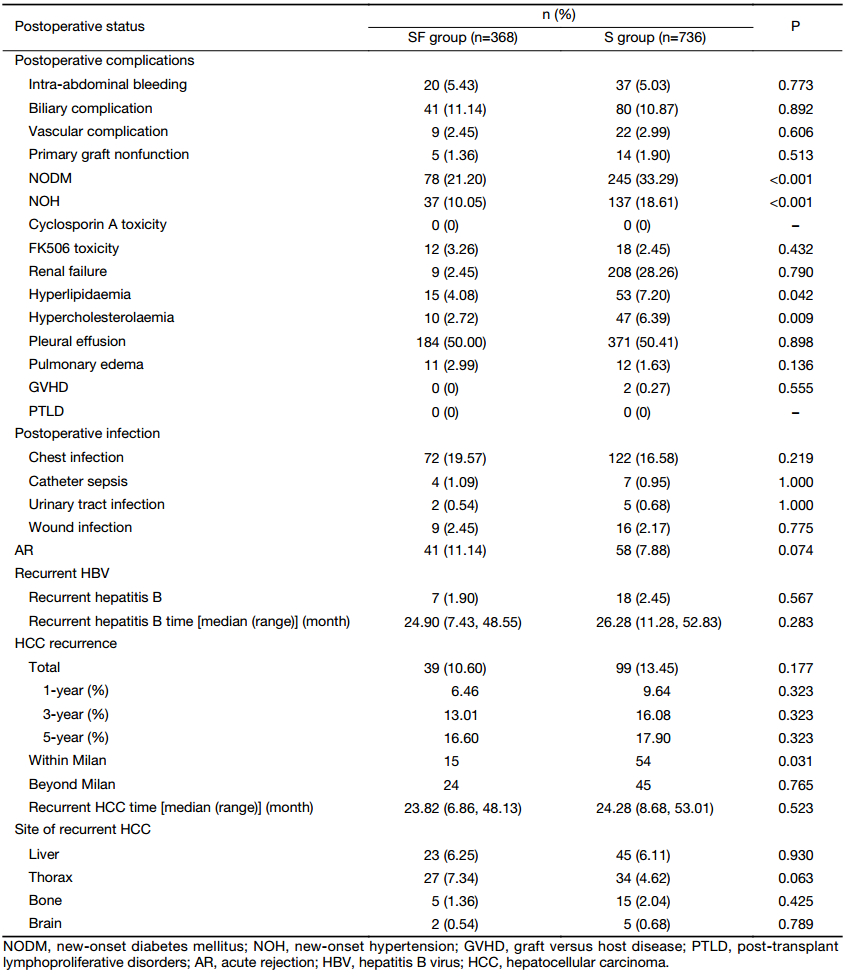
A total of 41 of the 368 patients (11.14%) in the SF group had histologically confirmed AR episodes by three months after LT. A first histologically confirmed AR episode was reported in 58 (7.88%) of the 736 patients in the S group. The difference in AR incidence between the SF group and the S group did not reach statistical significance (P=0.074) (Table 2). The occurred periods of AR were also similar: 0.56 (range: 0.26, 1.09) months in the SF group and 0.95 (range: 0.41, 6.18) months in the S group (P=0.086). In all of the cases, the AR was treated by bolus steroid administration and by increasing the trough level of the CNI (Table 3).
Full table
Full table
HBV recurrence
The HBV recurrence rate was 1.90% (7/368) in the SF group and 2.45% (18/736) in the S group (P=0.567). The mean interval for the development of HBV recurrence was 24.90 (range, 7.43–48.55) months in the SF group and 26.28 (range, 11.28–52.83) months in the S group (P=0.283) (Table 2). There were no significant differences in 1-year, 3-year or 5-year overall HBV recurrence rates (1.55% vs. 0.89%, 2.05% vs. 3.16% and 2.92% vs. 4.02%, P=0.634) between the two groups.
HCC recurrence
There were no differences in 1-year, 3-year and 5-year HCC recurrence rates between the S group and SF group (9.64% vs. 6.46%, 16.08% vs. 13.01% and 17.90% vs. 16.60%, P=0.323) (Table 2).
Two hundred and forty patients in the S group and 479 patients in the SF group fulfilled the Milan criteria (P=0.964). For patients who fulfilled the Milan criteria, the 1-year, 3-year and 5-year HCC recurrence rates (2.57% vs. 8.39%, 7.34% vs.13.50% and 8.66% vs. 14.55%, P=0.046) were significantly lower in the SF group than in the S group. The 1-year, 3-year and 5-year HCC recurrence rates (13.71% vs. 11.94%, 24.27% vs. 20.84% and 35.31% vs. 24.33%, P=0.386) of patients exceeding the Milan criteria showed no significant differences between the S group (n=128) and the SF group (n=257).
Clinical factors related to tumor recurrence in steroid avoidance recipients
Table 4 summarizes the characteristics of SF group. The recipients who experienced more tumor recurrence were younger, more with HBV DNA >1,000 copies/mL and more beyond Milan criteria (P=0.028, P<0.001 and P<0.001, respectively). Recipients’ age, HBV DNA >1,000 copies/mL and beyond Milan criteria were significantly correlated to tumor recurrence in univariate analysis. They were entered into multivariate logistic regression (Table 5), which indicates that the recipients with younger age [odds ratio (OR), 1.053; P=0.011], preoperative HBV DNA ≥1,000 copies/mL (OR, 2.597; P=0.004) and beyond Milan criteria (OR, 4.255; P<0.001) were identified as the risk factors associated with tumor recurrence in steroid avoidance recipients after LT.
Full table

Full table
Survival
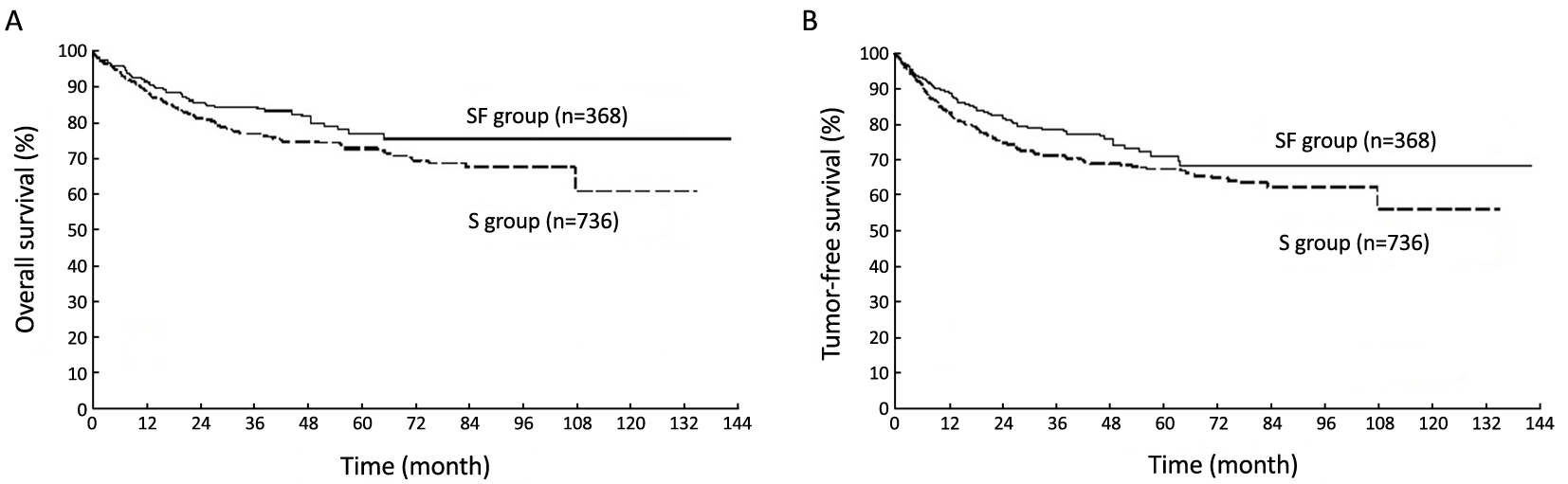
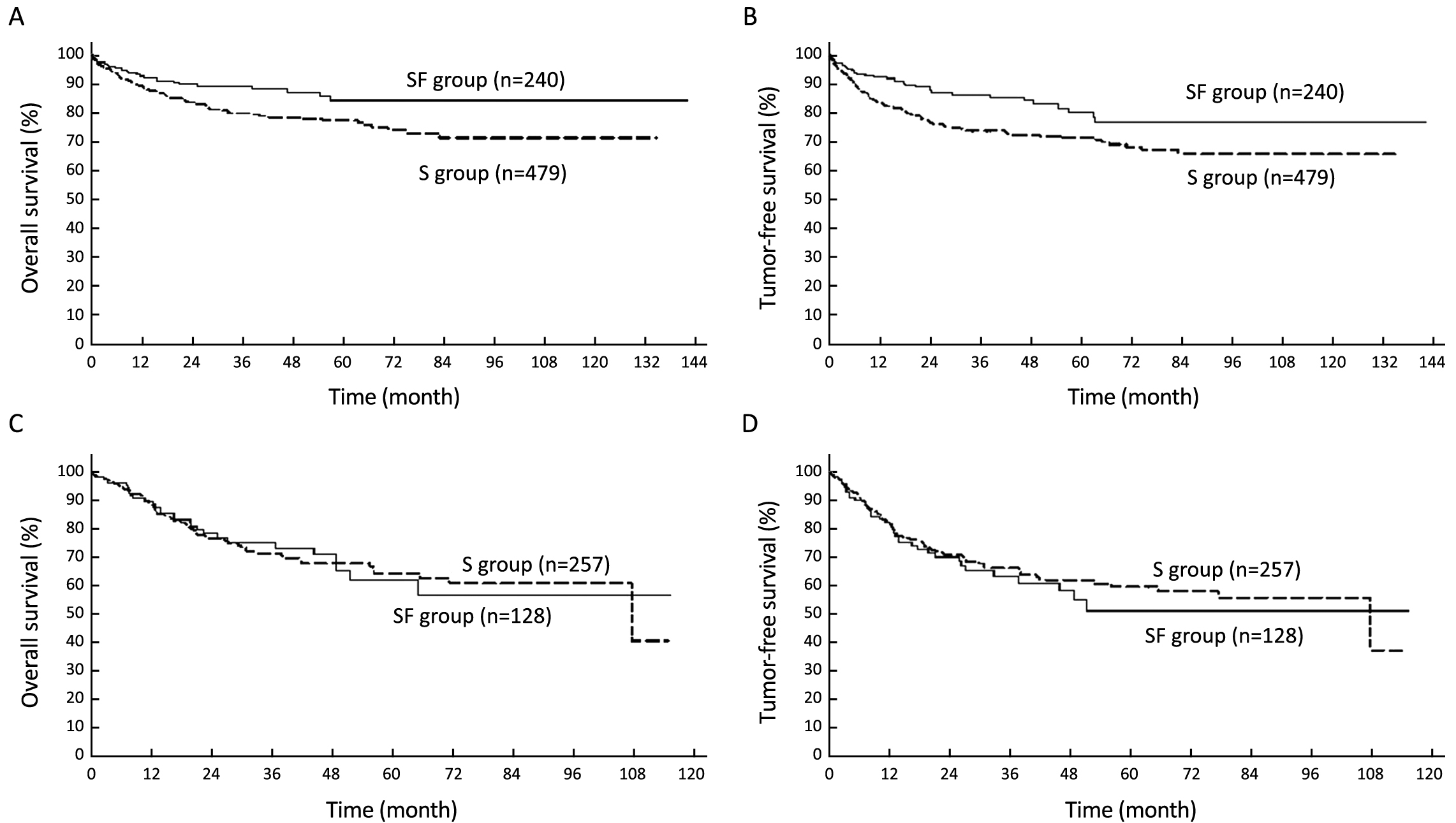
Compared with the S group, the SF group showed significantly higher OS (P=0.043) and TFS curves (P=0.048) (Figure 2). For patients who fulfilled the Milan criteria, the OS (P=0.013) and TFS (P=0.004) curves were significantly higher in the SF group than in the S group (Figure 3A, B). For patients exceeding the Milan criteria, the OS (P=0.945) and TFS (P=0.596) curves showed no significant differences between the SF group and the S group (Figure 3C, D).
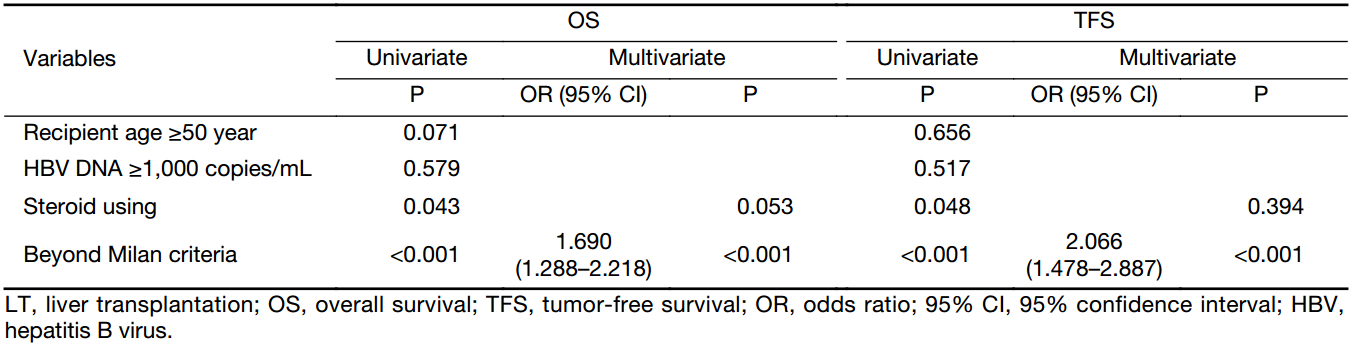
We evaluated factors that influenced the OS and TFS (Table 6). In the univariate analysis, steroid using (P=0.043 and P=0.048) and beyond Milan criteria (P<0.001 for both) were significantly associated with recipient OS and TFS. Factors associated with P<0.05 in the univariate analysis were entered into a multivariate analysis using Cox regression. In the multivariate analysis, recipient beyond Milan criteria was an independent prognostic factor for OS (OR, 1.690; P<0.001) and TFS (OR, 2.066; P<0.001) after LT.
Full table
Other post-LT complications
Compared to the S group, the SF group was associated with significantly lower incidences of NODM (21.20% vs. 33.29%, P<0.001), new-onset hypertension (NOH) (10.05% vs. 18.61%, P<0.001) and hyperlipidemia (4.08% vs. 7.20%, P=0.042) after LT (Table 2).
Discussion
Several IS protocols without steroids have recently been reported in China (8,17,18); however, the majority of these trials have been single-center research studies with small numbers of cases. Our study was the first multiple-center research focused on such a large number of HBV-related HCC patients in China, leading to more accurate and credible results.
As we know, the prevention of rejection is the initial purpose of steroids use. Steroids inhibit prostaglandin synthesis, inhibit IL-1 transcription and IL-1-dependent lymphocyte activation, stabilize lysosomal membranes and reduce histamine and bradykinin release (25). Therefore, safety is the premise of a steroid-free IS regimen. Early steroid avoidance in LT showed a high incidence of AR (26). Basiliximab is a chimeric monoclonal antibody with high affinity for the CD25 chain of the interleukin-2 receptor. It has already been shown that addition of basiliximab to conventional IS therapy provided increased efficacy in reducing the incidence of AR, with no clinically significant increases in adverse events (27,28). Basiliximab at a dose of 20 mg on d 0 and d 4 achieved consistent suppression of CD25 for a period of 30 to 45 d, without the risk of prolonged immunosuppression (29). In the present study, we also used basiliximab in the SF group and detected no difference in AR rate between the two groups, which is consistent with most previous studies (30,31).
A multicenter study provided evidence that steroids play an important role in HCC tumor recurrence after LT (10). Steroids may contribute to tumor recurrence. The potential mechanism for steroids contributing to tumor recurrence may be that steroids might reduce the potency of immune inflammatory response or inhibit malignant-cell apoptosis and promote migration of these cells (32-34). Although in the present study, the tumor recurrence rates in the S group were not higher than those in the SF group, we found in patients within the Milan criteria, both the OS and TFS rates were higher in patients receiving steroid-free immunosuppression compared with those using steroid protocols. On the other hand, there were no differences of both the OS and TFS curves between the patients beyond Milan criteria with or without steroid treatment. This result indicated that Milan criteria maybe an important factor that affecting recipient’s prognosis. Our multivariate analysis showed recipient beyond Milan criteria was an independent prognostic factor for OS and TFS after LT which confirmed the above hypothesis.
In this study, we observed that the HBV recurrence was more than double in the steroid group, although there were no statistically significant differences. This may be due to, at least in part, different samples sizes. How certain IS regimens influence HBV recurrence is not clear. There has been consideration that steroid-free IS therapy in HBV patients results in better long-term outcomes regarding HBV recurrence. A multicenter study from South Korea showed that the cumulative steroid dose was a risk factor for HBV recurrence, which could be explained by HBV having a corticosteroid receptor that promotes virus replication (35). Currently, most of the researches on steroid-free have been nonrandomized and retrospective, inevitably having some flaws. Further larger prospective, randomized studies are required to understand the underlying molecular mechanisms that influence how certain IS regimens influence HBV recurrence in the transplant recipients.
In this study, the SF group is an independent sample. All the recipients in S group were matched with those in SF group, so the S group is not an independent sample. This is the reason why a multivariate analysis is carried out only in SF group. The result indicates that age, pretransplant HBV DNA level and Milan criteria were identified as the major risk factors associated with tumor recurrence in steroid avoidance recipients after LT. Younger age was related to early recurrence after curative resection in HCC in some researches but not independent risk factor (36). While in another study, age >57 years was an independent predictor of HCC recurrence after LT (37). The analysis in our study is based on steroid avoidance, which is different from the above studies. The role of age in HCC recurrence of steroid avoidance recipients should be further resolved.
Accumulating evidence has shown that for patients with HBV infection, high serum HBV DNA level before tumor resection is a strong predictor of HCC recurrence (38-40), which is consistent with our finding. Exceeding Milan criteria has proven to be a discerning prognostic tool in the prediction of HCC recurrence after LT. The results suggest that these three factors should be got into account in our choice of no steroid recipients.
Reducing the metabolic complications that otherwise increase the risk of morbidity and mortality from cardiovascular events is another main objective of steroid-free IS regimens (11). As in previous studies, the avoidance of steroids resulted in a significant reduction in the incidences of NODM, post-transplant hypercholesterolemia and hypertriglyceridemia (41). Comparing the rates of all metabolic side effects (NODM, dyslipidemia and NOH), there was a trend toward more metabolic impairment in the S group, compared to the SF group. This finding might constitute evidence that steroid avoidance is beneficial for long-term metabolism following LT, compared to delayed steroid reduction.
Conclusions
Steroid-free immunosuppression could be safe and feasible for HBV-related HCC patients in LT. Age, HBV DNA level and Milan criteria may be risk factors associated with tumor recurrence in steroid avoidance recipients. Recipient beyond Milan criteria was an independent prognostic factor and recipient fulfilling Milan criteria can benefit the most from steroid-free immunosuppression.
Acknowledgements
We gratefully acknowledge the CLTR for the data collection and statistical analysis. We also acknowledge the transplant centers from mainland China for their major contribution to the CLTR database. This work was supported by the Cheung Kong Scholars Program, the Zhejiang Provincial Program for the Cultivation of High-level Innovative Health Talents and the Projects of Medical and Health Technology Program in Zhejiang Province (No. 2015KYB151 and 2017RC002).
Footnote
Conflicts of Interest: The authors have no conflicts of interest to declare.
References
- Chen W, Zheng R, Zuo T, et al. National cancer incidence and mortality in China, 2012. Chin J Cancer Res 2016;28:1–11. DOI:10.3978/j.issn.1000-9604.2016.02.08
- Ma X, Yang Y, Tu H, et al. Risk prediction models for hepatocellular carcinoma in different populations. Chin J Cancer Res 2016;28:150–60. DOI:10.21147/j.issn.1000-9604.2016.02.02
- Yang Y, Sun JW, Zhao LG, et al. Quantitative evaluation of hepatitis B virus mutations and hepatocellular carcinoma risk: a meta-analysis of prospective studies. Chin J Cancer Res 2015;27:497–508. DOI:10.3978/j.issn.1000-9604.2015.10.05
- Yang PC, Ho CM, Hu RH, et al. Prophylactic liver transplantation for high-risk recurrent hepatocellular carcinoma. World J Hepatol 2016;8:1309–17. [PubMed] DOI:10.4254/wjh.v8.i31.1309
- Chapman WC, Garcia-Aroz S, Vachharajani N, et al. Liver transplantation for advanced hepatocellular carcinoma after downstaging without up-front stage restrictions. J Am Coll Surg 2017;224:610–21. [PubMed] DOI:10.1016/j.jamcollsurg.2016.12.020
- Zaydfudim VM, Pelletier SJ. Towards steroid-free immunosuppression after liver transplantation. Gut Liver 2016;10:495–6. [PubMed] DOI:10.5009/gnl16204
- Ho WL, Wu CC, Yeh DC, et al. Roles of the glucocorticoid receptor in resectable hepatocellular carcinoma. Surgery 2002;131:19–25. [PubMed] DOI:10.1067/msy.2002.118710
- Wei Q, Xu X, Wang C, et al. Efficacy and safety of a steroid-free immunosuppressive regimen after liver transplantation for hepatocellular carcinoma. Gut Liver 2016;10:604–10. [PubMed] DOI:10.5009/gnl15017
- Gündisch S, Boeckeler E, Behrends U, et al. Glucocorticoids augment survival and proliferation of tumor cells. Anticancer Res 2012;32:4251–61. [PubMed]
- Mazzaferro V, Rondinara GF, Rossi G, et al. Milan multicenter experience in liver transplantation for hepatocellular carcinoma. Transplant Proc 1994;26:3557–60. [PubMed]
- Keeffe EB. Liver transplantation: current status and novel approaches to liver replacement. Gastroenterology 2001;120:749–62. [PubMed] DOI:10.1053/gast.2001.22583
- Marubashi S, Dono K, Amano K, et al. Steroid-free living-donor liver transplantation in adults. Transplantation 2005;80:704–6. [PubMed]
- Perkins J. Adrenal failure in liver transplant patients: does steroid-free immunosuppression place recipients at risk for an adrenal crisis?. Liver Transpl 2006;12:160–2. [PubMed]
- Shigeta T, Sakamoto S, Uchida H, et al. Basiliximab treatment for steroid-resistant rejection in pediatric patients following liver transplantation for acute liver failure. Pediatr Transplant 2014;18:860–7. [PubMed] DOI:10.1111/petr.12373
- Klintmalm GB, Washburn WK, Rudich SM, et al. Corticosteroid-free immunosuppression with daclizumab in HCV(+) liver transplant recipients: 1-year interim results of the HCV-3 study. Liver Transpl 2007;13:1521–31. [PubMed] DOI:10.1002/lt.21182
- Sen S, Dawwas MF, Nash KL, et al. Uncomplicated strongyloidiasis in a liver transplant recipient on steroid-free immunosuppression. Transpl Infect Dis 2010;12:184–5. [PubMed] DOI:10.1111/j.1399-3062.2009.00462.x
- Liu YY, Li CP, Huai MS, et al. Comprehensive comparison of three different immunosuppressive regimens for liver transplant patients with hepatocellular carcinoma: steroid-free immunosuppression, induction immunosuppression and standard immunosuppression. PLoS One 2015;10:e0120939. [PubMed] DOI:10.1371/journal.pone.0120939
- Hu AB, Wu LW, Tai Q, et al. Safety and efficacy of four steroid-minimization protocols in liver transplant recipients: 3-year follow-up in a single center. J Dig Dis 2013;14:38–44. [PubMed] DOI:10.1111/1751-2980.12008
- Zheng SS, Xu X, Wu J, et al. Liver transplantation for hepatocellular carcinoma: Hangzhou experiences. Transplantation 2008;85:1726–32. [PubMed] DOI:10.1097/TP.0b013e31816b67e4
- Linden A. A comparison of approaches for stratifying on the propensity score to reduce bias. J Eval Clin Pract 2017;23:690–6. [PubMed] DOI:10.1111/jep.12701
- Zheng S, Chen Y, Liang T, et al. Prevention of hepatitis B recurrence after liver transplantation using lamivudine or lamivudine combined with hepatitis B Immunoglobulin prophylaxis. Liver Transpl 2006;12:253–8. [PubMed] DOI:10.1002/lt.20701
- Ling Q, Wang K, Lu D, et al. Major influence of renal function on hyperlipidemia after living donor liver transplantation. World J Gastroenterol 2012;18:7033–9. [PubMed] DOI:10.3748/wjg.v18.i47.7033
- Ling Q, Xie H, Lu D, et al. Association between donor and recipient TCF7L2 gene polymorphisms and the risk of new-onset diabetes mellitus after liver transplantation in a Han Chinese population. J Hepatol 2013;58:271–7. [PubMed] DOI:10.1016/j.jhep.2012.09.025
- Taylor AL, Watson CJ, Bradley JA. Immunosuppressive agents in solid organ transplantation: Mechanisms of action and therapeutic efficacy. Crit Rev Oncol Hematol 2005;56:23–46. [PubMed] DOI:10.1016/j.critrevonc.2005.03.012
- Rolles K, Davidson BR, Burroughs AK. A pilot study of immunosuppressive monotherapy in liver transplantation: tacrolimus versus microemulsified cyclosporin. Transplantation 1999;68:1195–8. [PubMed] DOI:10.1097/00007890-199910270-00021
- Marino IR, Doria C, Scott VL, et al. Efficacy and safety of basiliximab with a tacrolimus-based regimen in liver transplant recipients. Transplantation 2004;78:886–91. [PubMed] DOI:10.1097/01.TP.0000134970.92694.68
- Gruttadauria S, Cintorino D, Piazza T, et al. A safe immunosuppressive protocol in adult-to-adult living related liver transplantation. Transplant Proc 2006;38:1106–8. [PubMed] DOI:10.1016/j.transproceed.2006.02.141
- Calmus Y, Scheele JR, Gonzalez-Pinto I, et al. Immunoprophylaxis with basiliximab, a chimeric anti-interleukin-2 receptor monoclonal antibody, in combination with azathioprine-containing triple therapy in liver transplant recipients. Liver Transpl 2002;8:123–31. [PubMed] DOI:10.1053/jlts.2002.30882
- Moench C, Barreiros AP, Schuchmann M, et al. Tacrolimus monotherapy without steroids after liver transplantation -- a prospective randomized double-blinded placebo-controlled trial. Am J Transplantation 2007;7:1616–23. [PubMed] DOI:10.1111/j.1600-6143.2007.01804.x
- Kim JM, Joh JW, Kim SJ, et al. Steroid withdrawal in adult liver transplantation: occurrence at a single center. Transplant Proc 2010;42:4132–6. [PubMed] DOI:10.1016/j.transproceed.2010.10.018
- Cronstein BN, Kimmel SC, Levin RI, et al. A mechanism for the antiinflammatory effects of corticosteroids: the glucocorticoid receptor regulates leukocyte adhesion to endothelial cells and expression of endothelial-leukocyte adhesion molecule 1 and intercellular adhesion molecule 1. Proc Natl Acad Sci U S A 1992;89:9991–5. [PubMed]
- Brattsand R, Linden M. Cytokine modulation by glucocorticoids: mechanisms and actions in cellular studies. Aliment Pharmacol Ther 1996;10 Suppl 2:81–90. [PubMed]
- Yazawa H, Kato T, Nakada T, et al. Glucocorticoid hormone suppression of human neutrophil-mediated tumor cell cytostasis. Int J Cancer 1999;81:74–80. [PubMed] DOI:10.1002/(SICI)1097-0215(19990331)81:1<74::AID-IJC14>3.0.CO;2-S
- Yi NJ, Suh KS, Cho JY, et al. Recurrence of hepatitis B is associated with cumulative corticosteroid dose and chemotherapy against hepatocellular carcinoma recurrence after liver transplantation. Liver Transpl 2007;13:451–8. [PubMed] DOI:10.1002/lt.21043
- Zhou L, Rui JA, Wang SB, et al. Early recurrence in large hepatocellular carcinoma after curative hepatic resection: prognostic significance and risk factors. Hepatogastroenterology 2014;61:2035–41. [PubMed] DOI:10.5754/hge13772
- Senkerikova R, Frankova S, Sperl J, et al. Incidental hepatocellular carcinoma: risk factors and long-term outcome after liver transplantation. Transplant Proc 2014;46:1426–9. [PubMed] DOI:10.1016/j.transproceed.2014.03.010
- Chuma M, Hige S, Kamiyama T, et al. The influence of hepatitis B DNA level and antiviral therapy on recurrence after initial curative treatment in patients with hepatocellular carcinoma. J Gastroenterol 2009;44:991–9. [PubMed] DOI:10.1007/s00535-009-0093-z
- Huang L, Li J, Lau WY, et al. Perioperative reactivation of hepatitis B virus replication in patients undergoing partial hepatectomy for hepatocellular carcinoma. J Gastroenterol Hepatol 2012;27:158–64. [PubMed] DOI:10.1111/j.1440-1746.2011.06888.x
- Yang T, Lu JH, Zhai J, et al. High viral load is associated with poor overall and recurrence-free survival of hepatitis B virus-related hepatocellular carcinoma after curative resection: a prospective cohort study. Eur J Surg Oncol 2012;38:683–91. [PubMed] DOI:10.1016/j.ejso.2012.04.010
- Stegall MD, Everson GT, Schroter G, et al. Prednisone withdrawal late after adult liver transplantation reduces diabetes, hypertension, and hypercholesterolemia without causing graft loss. Hepatology 1997;25:173–7. [PubMed] DOI:10.1002/hep.510250132
- Everson GT, Trouillot T, Wachs M, et al. Early steroid withdrawal in liver transplantation is safe and beneficial. Liver Transpl Surg 1999;5(4 Suppl 1):S48–57. [PubMed] DOI:10.1053/JTLS005s00048