
Trends of incidence rate and age at diagnosis for cervical cancer in China, from 2000 to 2014
Introduction
Cervical cancer is the fourth most common cancer affecting women worldwide, after breast, colorectal, and lung cancers (1). There were an estimated 527,600 new cervical cancer cases and 265,700 deaths worldwide in 2012 (1). China accounted for 18.8% of new cervical cancer cases (99,000) and 9.4% of cervical cancer deaths (25,000) in 2012 (2). Furthermore, an estimated 98,900 cases of cervical cancer were diagnosed, and an estimated 30,500 women died attributable to cervical cancer in China in 2015 (3). The heavy burden of cervical cancer accounted for high medical costs. The total payments on cervix uteri and corpus uteri cancer treatments in China were estimated to be 11.5 billion RMB in 2015 (4).
In contrast to favorable overall decreasing trends in many countries (1), the incidence and mortality rates of cervical cancer were on the rise in China (2,5,6). The same as large geographic variations in cervical cancer incidence rates in the world (7), a disparity also exists between urban and rural China (5). In addition, a worldwide study on trends of cervical cancer incidence has found younger women are mostly affected by rising incidence in several countries including China, but the observation period was from 1990 to 2000 which was relatively short (1,8). The former epidemiological study at provincial level (9) and multicenter clinical study has found an increasing incidence of cervical cancer in young women (10,11). These studies had a bearing on their degree of national representativeness and would limit the evidences available to develop appropriate policies for cervical cancer control. In this study, the updated data based on population at the national level were used to reveal the trends of incidence rate and the changes of age at diagnosis for cervical cancer in China, thus to better inform prevention, early detection and treatment activities in cervical cancer in China.
Materials and methods
Data source
Overall 22 registries (11 in urban and 11 in rural), providing integrated data from 2000 to 2014 by the National Central Cancer Registry (NCCR) of China, were selected to calculate the incidence trend and age change of cervical cancer, with 32,457 cervical cancer cases from a population of 307,262,821 person-years (28,064 cases from 252,521,260 person-years in urban and 4,393 cases from 54,741,561 person-years in rural). International Classification of Diseases for Oncology, version 10 (ICD10) was used to classify the cancer cases. In this study, the code for cervical cancer is C53. The detailed variables of each case including year, patient age at diagnosis and region (rural or urban China) were collected. Individual registries provided annual population data in the respective areas to the NCCR of China. These data were sourced from local Public Security or Statistical Bureaus or from calculations based on census data.
Statistical analysis
In this study, we calculated the crude incidence rates (CIRs), age-specific incidence rate (from <30 to 80+, within 10-year groups), the age-standardized incidence rates (ASIRs), age percentage distributions (from 0 to 85+, within 5-year groups) and standardized age percentage distributions. Age percentage distributions are expressed as the percentage of the total number of cervical cancer cases falling into each five-year age group. We evaluated geographic disparities within age groups for each year by calculating incidence rate ratios (IRRs), comparing rates in urban China to those among rural China (the reference group). Trends of CIRs and ASIRs were analyzed using Joinpoint regression, which fitted up to the best model on a logarithmic scale to the trends in the annual rates. Joinpoint analyses were performed using the software which is called “Joinpoint Regression Program” from the Surveillance Research Program of the US National Cancer Institute (12). We examined the incidence trends using age-period-cohort analyses. For evaluating the trends of age at diagnosis in cervical cancer incidence, we calculated mean age at diagnosis and standardized mean age at diagnosis. World Segi’s population structure was used for age-standardized incidence rate, and standardized age percentage and standardized mean age at diagnosis. SAS software (Version 9.4; SAS Institute Inc., Cary, NC, USA) was used for data analysis.
Results
Temporal trends in incidence rates
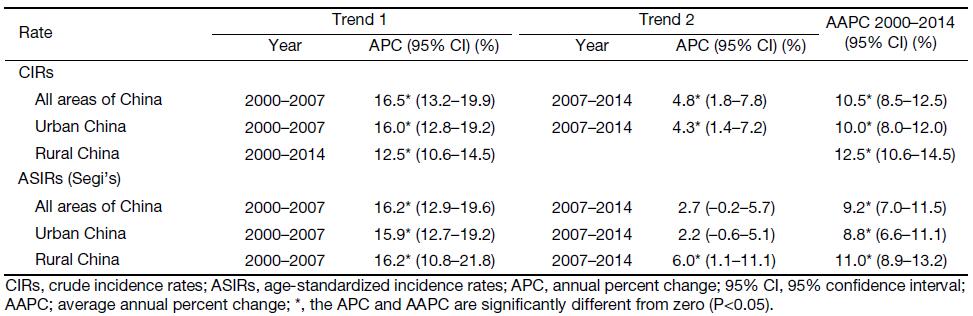
Table 1 illustrates the temporal trends of CIRs and ASIRs for cervical cancer in different areas of China. Generally speaking, there were significant increases for both CIRs and ASIRs in all areas and two regions of China. For CIRs, we found an overall significant increase in average annual percent change (AAPC) of incidence rate in all areas of China at 10.5% [95% confidence interval (95% CI): 8.5%–12.5%, P<0.05]. While the AAPC in rural areas was at 12.5% (95% CI: 10.6%–14.5%), the AAPC in urban areas was at 10.0% (95% CI: 8.0%–12.0%). After removing the influence of age structure, ASIRs showed the same patterns to CIRs, the AAPC of ASIRs in all areas of China was at 9.2% (95% CI: 7.0%–11.5%, P<0.05). While the AAPC in rural areas was at 11.0% (95% CI: 8.9%–13.2%), the AAPC in urban areas was at 8.8% (95% CI: 6.6%–11.1%). It was worthy to note that in 2000–2007, there was significant increase of ASIRs in both urban [annual percent change (APC)=15.9% (95% CI: 12.7%–19.2%)] and rural China [APC=16.2% (95% CI: 10.8%–21.8%)]. In 2007–2014, the ASIRs kept significantly increasing in rural China [APC=6.0% (95% CI: 1.1%–11.1%)], but it was nearly stable in urban China [APC=2.2% (95% CI: –0.6%–5.1%)].
Full table
Age-period-cohort analysis
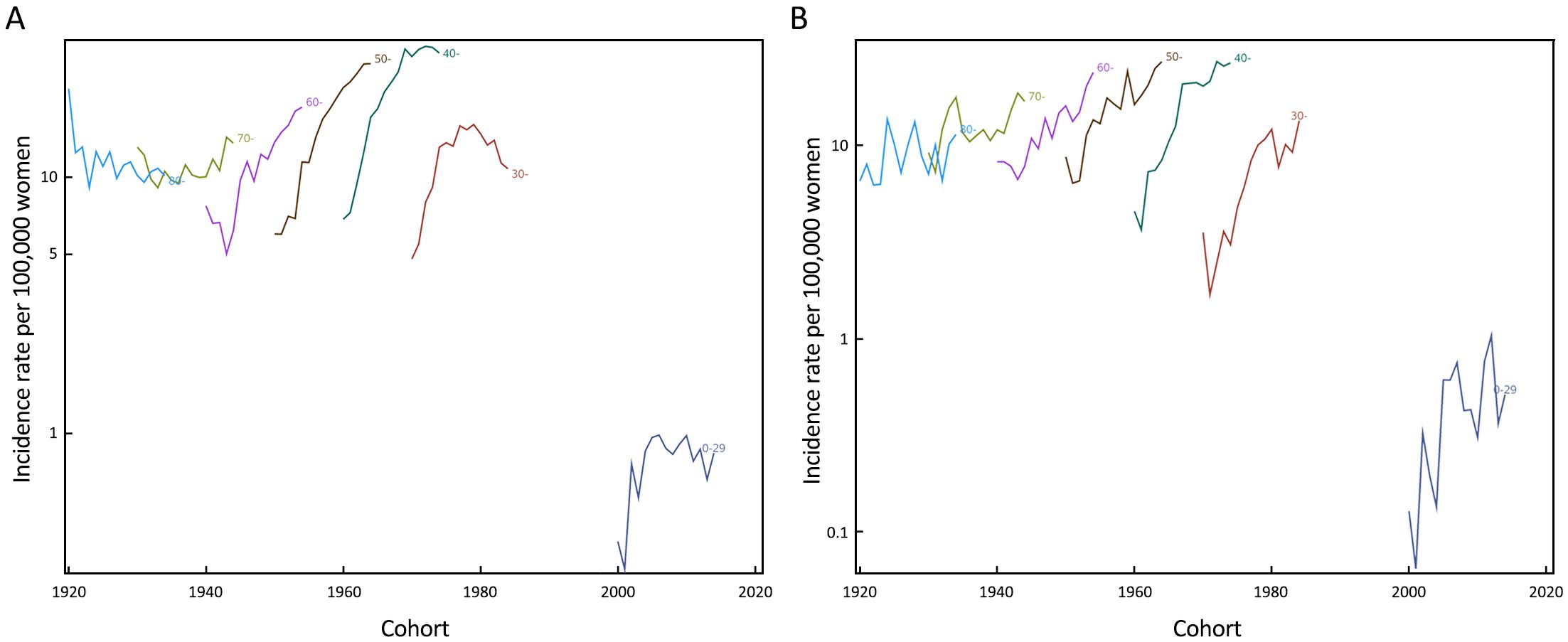
As shown in Figure 1A, CIRs and ASIRs for cervical cancer in urban and rural China generally showed sharp increasing trends during the period 2000–2014, except for ASIRs in urban China, which leveled off from 2009 to 2014. Taken together, CIRs and ASIRs in urban China were higher than CIRs and ASIRs in rural China during the whole observation period, respectively.
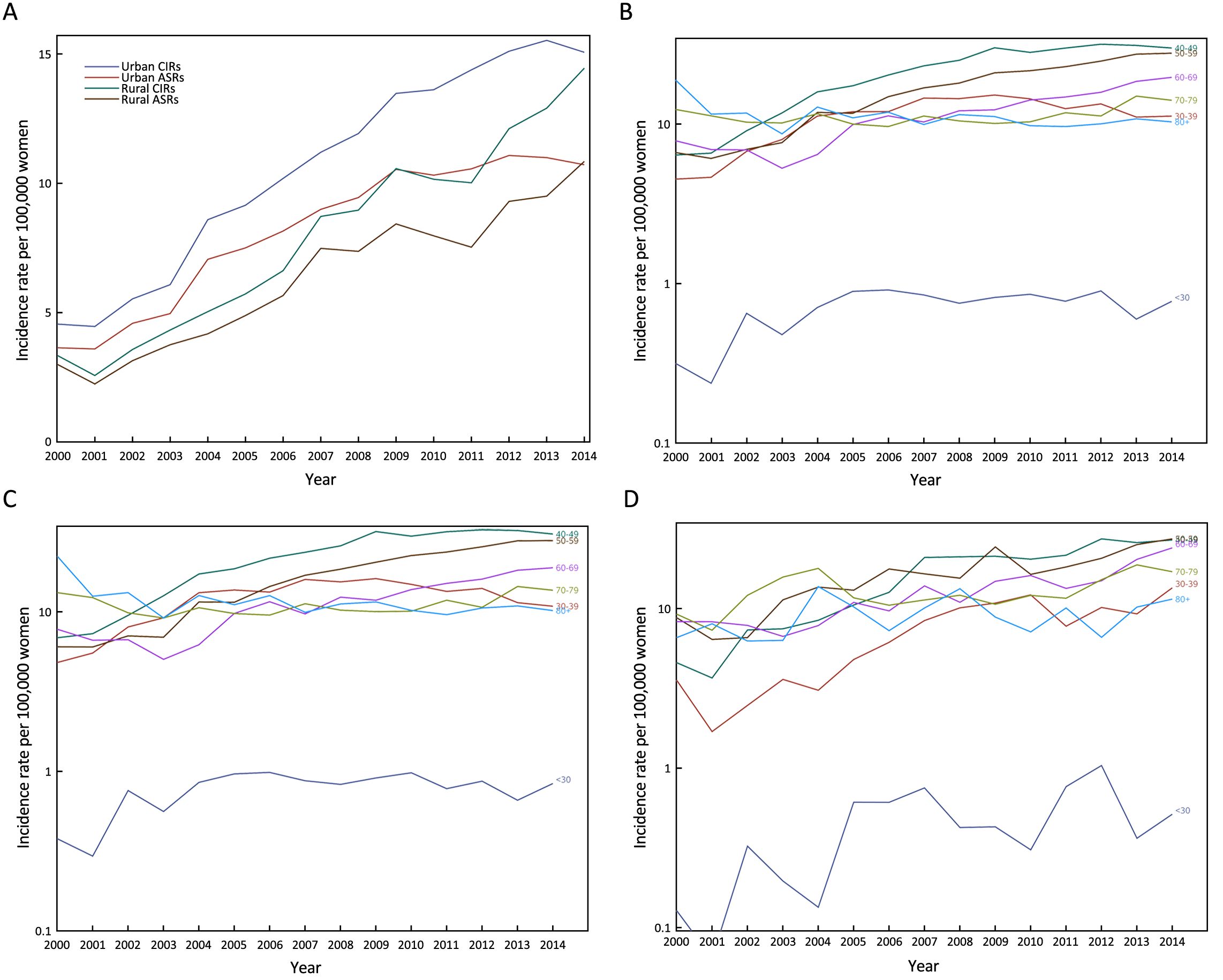
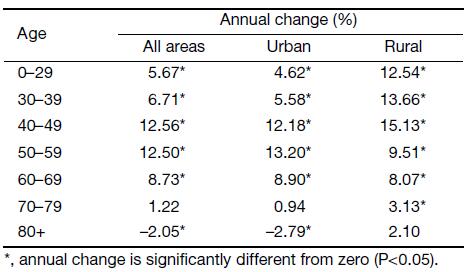
Annual changes of age-specific incidence rate are showed in Table 2. Generally speaking, the incidence rates in groups aged 0–69 years have significantly increased over time. In all areas of China and urban China, the APCs of groups aged 40–49 years and 50–59 years were more than 10%. In rural China, the APCs of groups aged 0–29, 30–39 and 40–49 years were more than 10%. Age-specific trends in incidence rates were plotted on a logarithmic scale in Figure 1B–1D. In all areas of China, urban China and rural China, the incidence rate in the age group younger than 30 years was always very low. In all areas of China and urban China, from 2000 to 2002, women aged 70+ years had higher incidence rate than those in other age groups. In rural China, from 2002 to 2004, women aged 70–79 years had higher incidence rate than those in other age groups. In all areas of China, with the rapid increase of incidence rate over time, women aged 40–49, 50–59 and 60–69 years were high-risk groups, and in particular, women aged 40–49 years showed the highest level of incidence rate from 2005 to 2014. Furthermore, Figure 2 shows the disparity of age-specific incidence rates between urban and rural China. Overall, the IRRs in younger age groups were higher than that in older age groups, and showed generally declined trends. For each age group, it got close to 1 over time. For instance, in women aged 0–29 years, the peak of IRRs reached 6.34 in 2004, but declined to 1.63 in 2014. In women aged 30–39 years, the peak of IRRs (4.29) also appeared in 2004, and then declined to 0.81. In women aged 40–49 years, the IRRs showed a gradually declined trend.
Full table
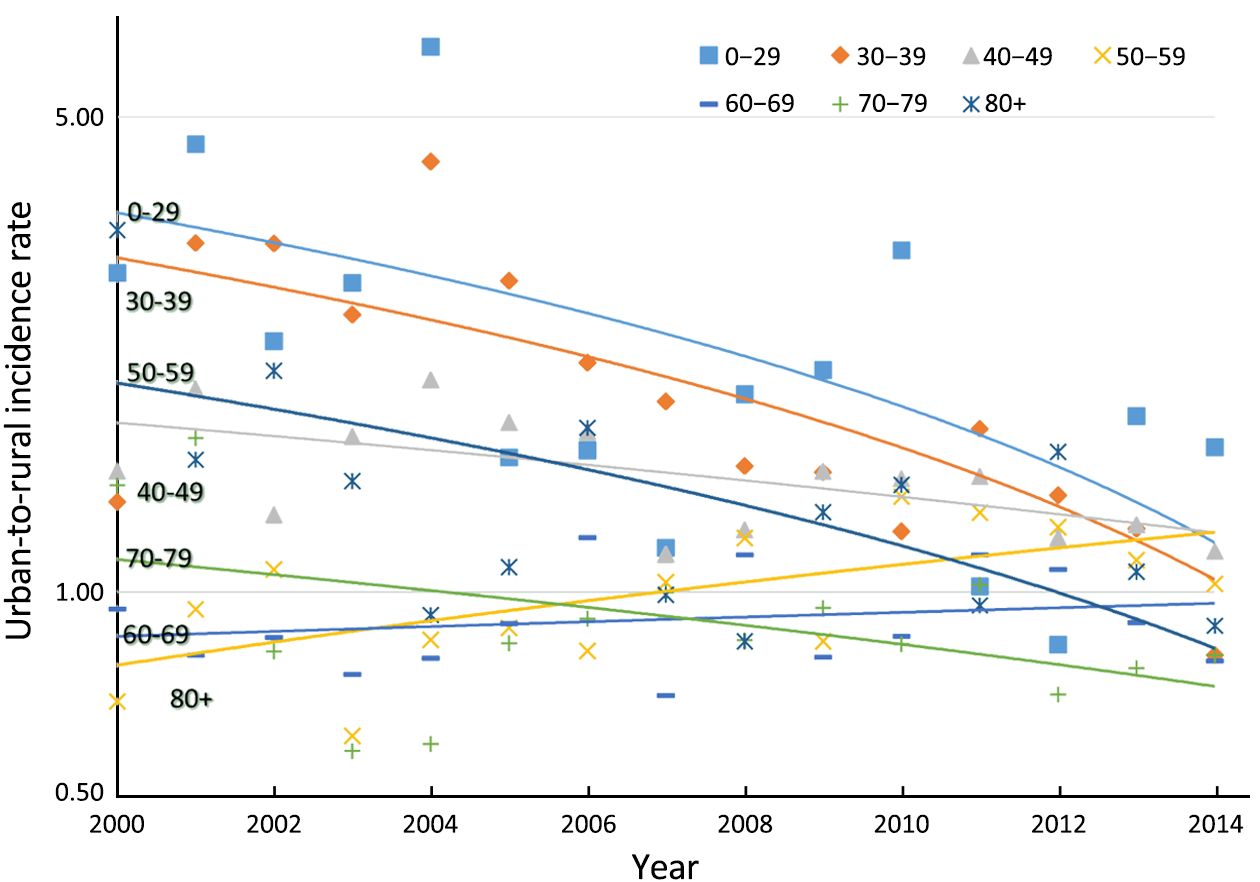
Figure 3 depicts the results of the birth cohort analysis. Generally speaking, there were clear generational effects in both urban and rural China. In urban China, an increasing risk of cervical cancer obviously existed in successive generations born from 1940 to 1970 followed by a weakened risk of cervical cancer in successive generations born from 1970 to 1990. In rural China, an increasing risk of cervical cancer obviously existed in successive generations born from 1940 to 1990.
Mean incidence age at diagnosis
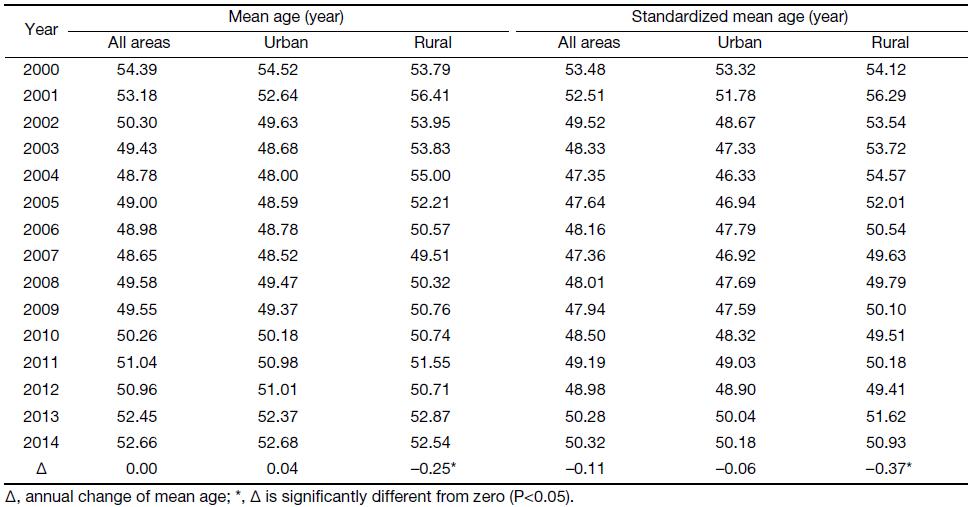
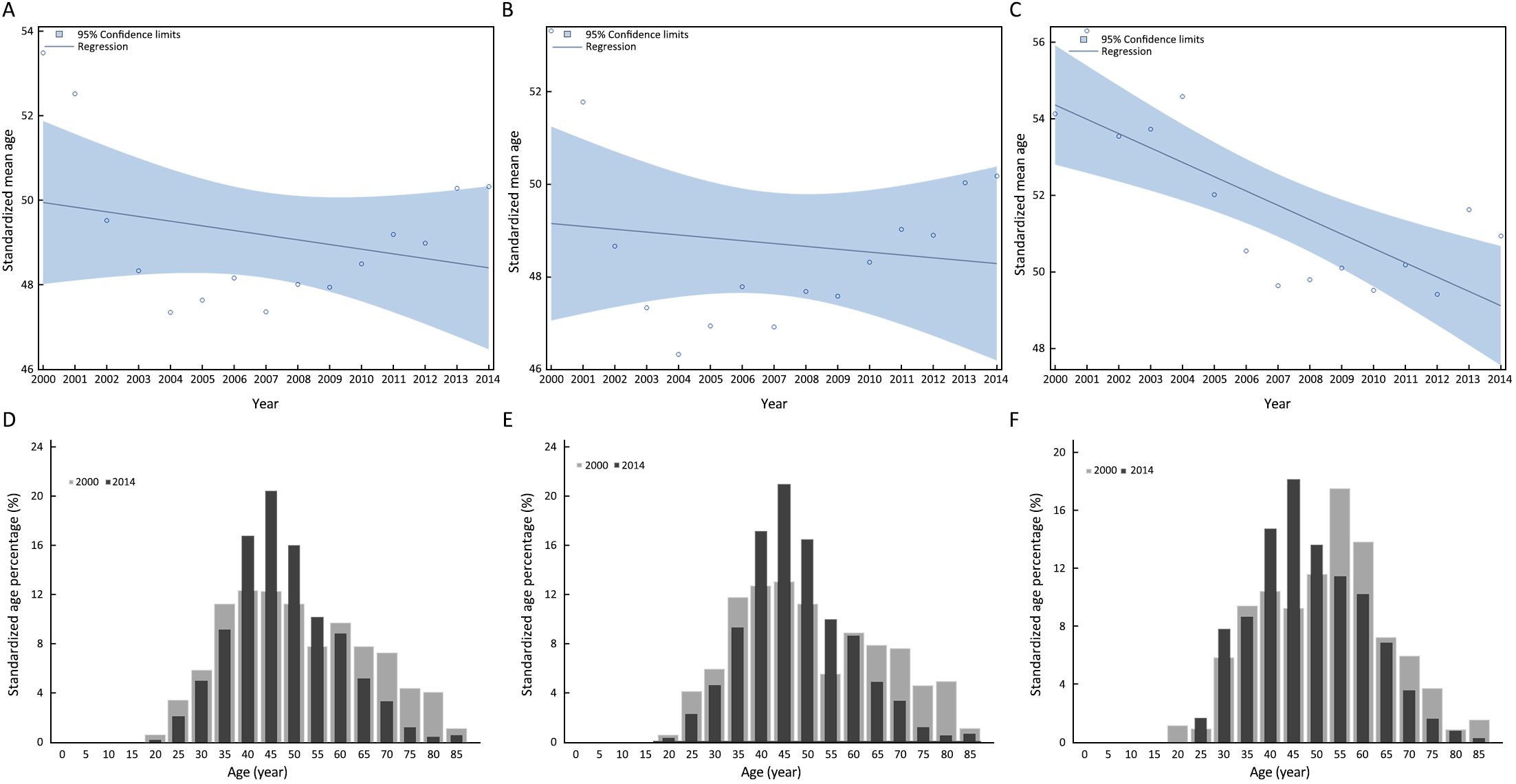
Table 3 and Figure 4A–4C show the trends of mean age and the standardized mean age at diagnosis for cervical cancer in China from 2000 to 2014. While the mean age at diagnosis kept steady in all areas of China during the observation period, the standardized mean age at diagnosis in all areas of China declined by 1.54 (0.11×14) years (Figure 4A), though the decline had no statistical significance. The decline trend of standardized mean age at diagnosis was more obvious in rural China than that in urban China. While the standardized mean age at diagnosis had dropped by 0.84 (0.06×14) years in urban China (Figure 4B), the standardized mean age at diagnosis had significantly declined by 5.18 (0.37×14) years in rural China (Figure 4C). In addition, the mean age at diagnosis in rural China also showed significantly declined.
Full table
Age composition at diagnosis
Figure 4D–4F depicts the comparison of standardized age percentages at diagnosis for cervical cancer in China between 2010 and 2014. In all areas of China and urban China, the main peak and secondary peak always appeared in the group aged 45–49 and 40–44 years. In urban China, the proportions of groups aged 40–59 years in 2014 were more than those in 2000, while the proportions of the rest groups in 2014 were less than those in 2000. In rural China, the main peak and secondary peak in 2000 appeared in the groups aged 55–59 and 60–64 years, respectively. In 2014, the main peak and secondary peak moved to the groups aged 45–49 and 40–44 years, respectively. The proportions of groups aged 25–34 and 40–54 years in 2014 were more than those in 2000, while the proportions of the rest groups in 2014 were less than those in 2000. Compared to the year 2000, the central tendency of age at diagnosis became more obvious in 2014 in all areas of China, and the groups aged 35–64 years constituted the main incidence population of cervical cancer. In urban China, the central tendency of age at diagnosis was more obvious than that in rural China. It was worthy to note that the proportion of groups aged 25–34 years also increased in rural China.
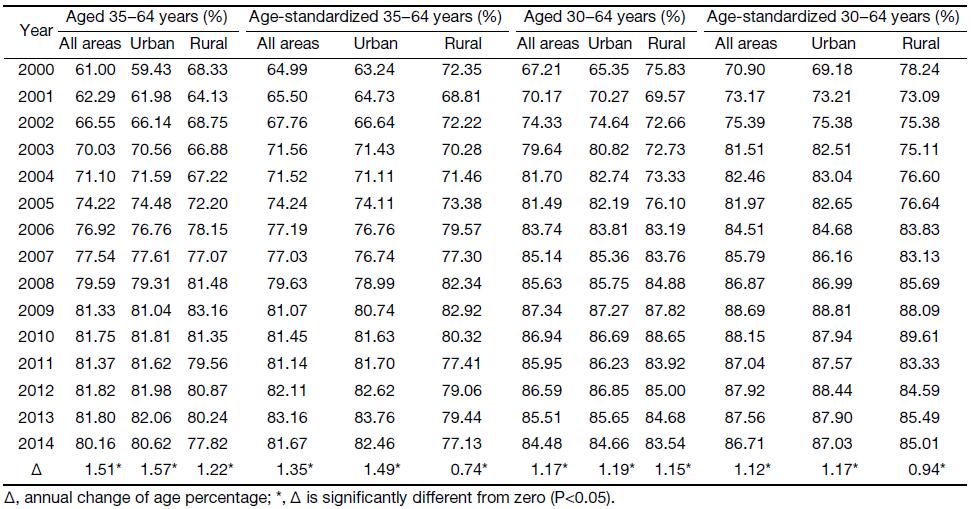
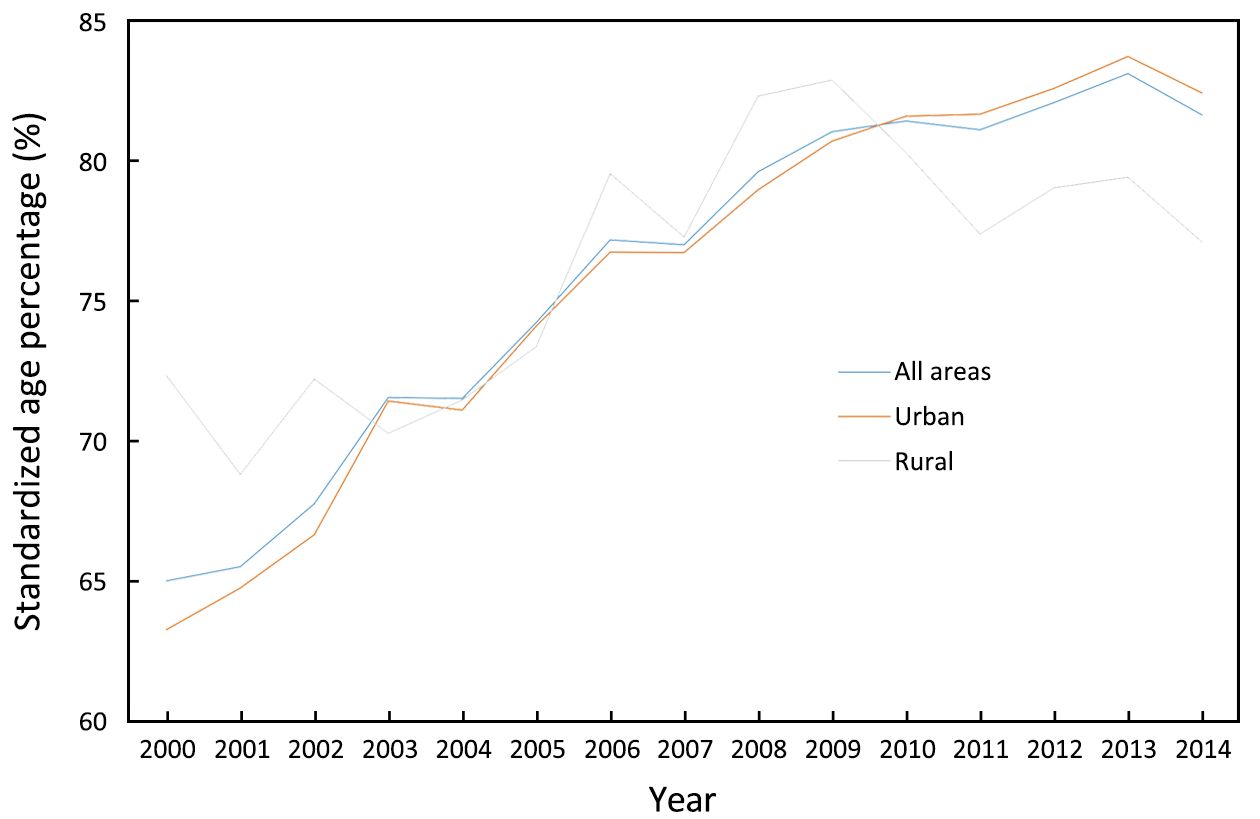
Table 4 shows the age percentages of women aged 35–64 and 30–64 years at diagnosis for cervical cancer in China from 2000 to 2014. Generally speaking, the age percentages and standardized age percentages have significantly increased in women aged 35–64 and 30–64 years. In all areas of China, the standardized age percentages of groups aged 35–64 and 30–64 years accounted for about 80% and 85%, respectively. Figure 5 shows the trends of standardized age percentages of women aged 35–64 years at diagnosis for cervical cancer in China from 2000 to 2014. Standardized age percentages of women aged 35–64 years in all areas of China has dramatically increased during the observation period. The trends of standardized age percentages of women aged 35–64 years in urban and rural China was the same as that in all areas of China, but the trend in rural China had a fluctuation.
Full table
Discussion
The findings of this study are as follows: 1) increased incidence rate for cervical cancer in China and narrowed gap in incidence rate between urban and rural China; 2) moved peak of incidence rate from groups aged 70+ years to group aged 40–49 years in all areas of China; 3) significantly dropped standardized mean age at diagnosis by 5.18 years in rural China; 4) moved peak of standardized age percentage from groups aged 55–64 years to groups aged 40–49 years in rural China; and 5) significant increases in standardized age percentages of women aged 35–64 years in China. Based on the above main findings, policy suggestions about increasing the uptake of screening and vaccination are proposed.
Incidence rate of cervical cancer kept increasing in China, and gap in incidence rate between urban and rural China was narrowed
While incidence rates of cervical cancer have fallen over the past decades in a number of countries (8), our study showed that China has kept sustained increasing trends from 2000 to 2014 and the trends were cohort-driven. The similar increasing trends were also observed in Zimbabwe, Uganda, Netherland and some countries of Central and Eastern Europe (8,13). Since high-risk human papillomavirus (HPV) types are considered a necessary cause of cervical cancer (14), the increasing trends of cervical cancer in China were mainly supposed to following reasons. One was the growing prevalence of high-risk HPV, which was reported to reach to 16.8% among female population in 1999–2008 (15). The other was the inadequacy of screening (3), which allows for the detection and removal of precancerous lesions, and HPV prevalence (13).
Although urban China had a higher incidence rate of cervical cancer than rural China from 2000 to 2014, rural China had relatively high increasing speed in cervical cancer incidence rate during this period. This geographic variation was due to differences in HPV prevalence (15) and the availability of screening (13). The IRRs declined and were closer to 1 in all age groups over time, which means that the previously observed gap in incidence rate of cervical cancer between urban and rural China was gradually narrowed. This is partly because in specific age groups, such as groups aged 40–49, 50–59 and 60–69 years, incidence rate in rural China had relatively high increasing speed. Moreover, from 2007 to 2014, while the incidence rate slightly dropped in urban women aged 30–39 years, the corresponding group was still increasing in rural China. The disparity of cohort effects between urban and rural China in generations born from 1970 to 1990 may be results of a combination of factors. Higher education (16), more awareness (1), better socioeconomic conditions (1) and bigger screening coverage (16) were considered meaningful in reduction of the cohort effects in urban China since 1970.
Change of mean age at diagnosis and age composition indicated trends of increasing cervical cancer incidence among younger women, especially in rural China
We found the peak of incidence rate was moved from groups aged 70+ years to group aged 40–49 years during the observation period, which was similar to former studies (10,11). A clear birth cohort effects found in this study may be a reasonable explanation, and this cohort-driven trend is thought to reflect increases in high-risk HPV prevalence from changing sexual behaviors (1,17). The phenomenon that the incidence rate of younger women was increasing not only existed in China, but also in Europe, Central Asian and Japan (1,8,18). The mean age at diagnosis (48.65–54.39 years) of cervical cancer in all areas of China from 2000 to 2014, was older than the median age at diagnosis (47–48 years) in USA and younger than the median age at diagnosis (55–59 years) in India (19). The mean age and median age at diagnosis for cervical cancer in this study were very close, but the data of median age at diagnosis were not exhibited.
On account of the fact that the mean age at diagnosis can be influenced by population structure, the change of mean age at diagnosis could be covered with the rapid population aging in China (20). Thus, we calculated the standardized mean age at diagnosis. By calculating the standardized mean age at diagnosis, we successfully removed the influence of population aging on trends of the mean age at diagnosis. The standardized mean age at diagnosis had significantly declined by 5.18 years in rural China, mainly because the standardized age percentage peak moved to the groups aged 45–49 and 40–44 years. The standardized age percentages of women aged 30–64 and 35–64 years in China showed significantly increasing trends, which confirmed the trends of increasing cervical cancer incidence among younger women in China.
Screening, vaccination and health education should be emphasized to reduce the increasing incidence rate of cervical cancer in China
Over the past 40 years, the incidence rate of cervical cancer has decreased by as much as 65% in some Western countries, where screening programs have been established (1). A recent study (16), which is the largest nationwide and population-based assessment of self-reported history of Papanicolaou (Pap) test for cervical cancer screening in China, has found that only one-fifth of Chinese women reported having ever had a Pap test. Moreover, women in rural areas were consistently less likely than women in urban areas to report having had a Pap test. Thus, the Pap test in China is inadequate, especially in rural areas.
To reduce the heavy burden contributed by cervical cancer, a free National Cervical Cancer Screening Program in Rural Areas (NCCSPRA) was launched by government in 221 counties since 1999 (21). The screening target age was set between 35 and 59 years at first three years, then was changed to 35–64 years up to now (21). According to our study, the screening age range set by NCCSPRA was basically reasonable, because the standardized age percentages of women aged 35–64 years was quite high at interval of 64.99%–83.16% from 2000 to 2014. However, an increasing proportion of women younger than 35 years was excluded from the program in rural China. The World Health Organization (WHO) recommends that all women between the ages of 30 and 49 years should be screened for cervical cancer at least once (22). In the EU member states, where the incidence rate was quite lower than China, screening usually starts at an age between 20 and 30 years and stops at age 60 to 70 years (23). Thus, based on this study and international experiences, we suggest that the lowest screening target age should be reduced by 5 years, which means the target age range should be continually broadened to 30–64 years. More importantly, the free National Cervical Cancer Screening Program, as a major public health project, should be expanded to all areas of China as early as possible in the face of increasing trends of incidence rate for cervical cancer.
There are several main barriers to participation in cervical cancer screening, including lack of knowledge and awareness of cervical cancer screening and its benefits, fear of pain and being diagnosed with cervical cancer, embarrassment, the lack of husband’s support for screening, and cultural factors (24,25). A recent study revealed that younger women were significantly more unwillingly to attend cervical cancer screening than older women in rural China, though they have a higher level of knowledge (26). A higher opportunity cost for younger women maybe a reasonable explanation for this behavior (26). Therefore, a relevant health education policy should be developed, which aimed at raising women’s awareness on the risk factors of cervical cancer and the importance of early diagnosis.
Since bivalent and quadrivalent HPV vaccine have received formal drug approval in mainland China in the past two years (27), which made population wide usage of HPV vaccine possible in China. To expand vaccination, a national level HPV vaccination strategy should be developed. Meanwhile, health education should be strengthened to raise public awareness on the efficacy of HPV vaccine in order to increase vaccine uptake. Moreover, the evaluation of HPV vaccine’s effectiveness and safety should be initiated.
Strengths, limitations and further needed studies are as follows
Strengths of our population-based analysis of the incidence trends and the changes of age at diagnosis for cervical cancer included our use of high-quality and long-term surveillance data from 22 oldest cancer registries in China. In addition, the observation period was relatively long (from 2000 to 2014). On account of the accurate and representative surveillance data, our results are convincing. Some specific limitations exist in this study. A major limitation is that the population covered by the rural areas of 22 cancer registries presented only a small sample, which lead to fluctuation in yearly incidence rate or age composition. Secondly, the age grouping maybe not the best, which lead to some useful information be covered. To better understand the trends of cervical cancer incidence, monitoring yearly data in the future need to be further emphasized. Besides, additional research is needed to determine the causality of factors involved in the disparity of cohort effects between urban and rural China.
Acknowledgements
This work was supported by Program Grant in Fundamental Research from the Ministry of Science and Technology (No. 2014FY121100) and Chinese Academy of Medical Sciences (CAMS) Innovation Fund for Medical Sciences (No. 201612M2004).
Footnote
Conflicts of Interest: The authors have no conflicts of interest to declare.
References
- Torre LA, Bray F, Siegel RL, et al. Global cancer statistics, 2012. CA Cancer J Clin 2015;65:87–108. DOI:10.3322/caac.21262
- Chen W, Zheng R, Zuo T, et al. National cancer incidence and mortality in China, 2012. Chin J Cancer Res 2016;28:1–11. DOI:10.3978/j.issn.1000-9604.2016.02.08
- Chen W, Zheng R, Baade PD, et al. Cancer statistics in China, 2015. CA Cancer J Clin 2016;66:115–32. DOI:10.3322/caac.21338
- Cai Y, Xue M, Chen W, et al. Expenditure of hospital care on cancer in China, from 2011 to 2015. Chin J Cancer Res 2017;29:253–62. DOI:10.21147/j.issn.1000-9604.2017.03.11
- Chen W, Zheng R, Zhang S, et al. Cancer incidence and mortality in China, 2013. Cancer Lett 2017;401:63–71. DOI:10.1016/j.canlet.2017.04.024
- Chen W, Zheng R, Zeng H, et al. Annual report on status of cancer in China, 2011. Chin J Cancer Res 2015;27:2–12. DOI:10.3978/j.issn.1000-9604.2015.01.06
- Pimple S, Mishra G, Shastri S. Global strategies for cervical cancer prevention. Curr Opin Obstet Gynecol 2016;28:4–10. DOI:10.1097/GCO.0000000000000241
- Vaccarella S, Lortet-Tieulent J, Plummer M, et al. Worldwide trends in cervical cancer incidence: impact of screening against changes in disease risk factors. Eur J Cancer 2013;49:3262–73. DOI:10.1016/j.ejca.2013.04.024
- Cai HB, Liu XM, Huang Y, et al. Trends in cervical cancer in young women in Hubei, China. Int J Gynecol Cancer 2010;20:1240–3.
- Wang T, Wu MH, Wu YM, et al. A population-based study of invasive cervical cancer patients in Beijing: 1993–2008. Chin Med J (Engl) 2015;128:3298–304. DOI:10.4103/0366-6999.171420
- Li S, Hu T, Lv W, et al. Changes in prevalence and clinical characteristics of cervical cancer in the People’s Republic of China: a study of 10,012 cases from a nationwide working group. Oncologist 2013;18:1101–7. DOI:10.1634/theoncologist.2013-0123
- Kim HJ, Fay MP, Feuer EJ, et al. Permutation tests for joinpoint regression with applications to cancer rates. Stat Med 2000;19:335–51.
- Torre LA, Siegel RL, Ward EM, et al. Global cancer incidence and mortality rates and trends -- an update. Cancer Epidemiol Biomarkers Prev 2016;25:16–27. DOI:10.1158/1055-9965.EPI-15-0578
- de Martel C, Ferlay J, Franceschi S, et al. Global burden of cancers attributable to infections in 2008: a review and synthetic analysis. Lancet Oncol 2012;13:607–15. DOI:10.1016/S1470-2045(12)70137-7
- Zhao FH, Lewkowitz AK, Hu SY, et al. Prevalence of human Papillomavirus and cervical intraepithelial neoplasia in China: a pooled analysis of 17 population-based studies. Int J Cancer 2012;131:2929–38. DOI:10.1002/ijc.27571
- Wang B, He M, Chao A, et al. Cervical cancer screening among adult women in China, 2010. Oncologist 2015;20:627–34. DOI:10.1634/theoncologist.2014-0303
- Forman D, de Martel C, Lacey CJ, et al. Global burden of human papillomavirus and related diseases. Vaccine 2012;30 Suppl 5:F12-23.
- Bray F, Lortet-Tieulent J, Znaor A, et al. Patterns and trends in human papillomavirus-related diseases in Central and Eastern Europe and Central Asia. Vaccine 2013;31 Suppl 7:H32-45.
- Ginsburg O, Bray F, Coleman MP, et al. The global burden of women’s cancers: a grand challenge in global health. Lancet 2017;389:847–60. DOI:10.1016/S0140-6736(16)31392-7
- Population Division of United Nations. World Population Ageing 2015. Available online: http://www.un.org/en/development/desa/population/publications/pdf/ageing/WPA2015_Report.pdf
- Di J, Rutherford S, Wu J, et al. Knowledge of cervical cancer screening among women across different socio-economic regions of China. PLoS One 2015;10:e0144819. DOI:10.1371/journal.pone.0144819
- World Health Organization. Comprehensive Cervical Cancer Control: A Guide to Essential Practice, 2nd edition. Geneva Switzerland Who, 2014.
- Anttila A, von Karsa L, Aasmaa A, et al. Cervical cancer screening policies and coverage in Europe. Eur J Cancer 2009;45:2649–58. DOI:10.1016/j.ejca.2009.07.020
- Nolan J, Renderos TB, Hynson J, et al. Barriers to cervical cancer screening and follow-up care among Black Women in Massachusetts. J Obstet Gynecol Neonatal Nurs 2014;43:580–8. DOI:10.1111/1552-6909.12488
- Williams M, Kuffour G, Ekuadzi E, et al. Assessment of psychological barriers to cervical cancer screening among women in Kumasi, Ghana using a mixed methods approach. Afr Health Sci 2013;13:1054–61. DOI:10.4314/ahs.v13i4.28
- Liu T, Li S, Ratcliffe J, et al. Assessing knowledge and attitudes towards cervical cancer screening among rural women in Eastern China. Int J environ Res Public Health 2017;14:pii:E967.
- Ji SS, Li KL, Li Y, et al. Progress toward development and use of prophylactic human papillomavirus vaccine. Zhongguo Yi Miao He Mian Yi (in Chinese) 2017;23:222–9.