
Cancer incidence in Beijing, 2014
Introduction
The fastest growing threat from non-communicable disease is considered to be the next health tsunami. As one of the major non-communicable diseases, cancer accounted for 1 in 6 and 1 in 4 deaths globally and China, respectively (1,2). Besides, it has been estimated that in 2012, 14.1 million and 3.1 million new cancer cases were diagnosed globally and in China according to GLOBOCAN 2012 (2). The epidemiologic pattern of cancer in Beijing is consistent with patterns in China and the world. In 2014, cancer was the leading cause of death in Beijing, which accounted for 27.1% of total deaths (3). Burden of disease from cancer is becoming one of the major public health issues. To resolve this issue, understanding the epidemiologic pattern of cancer, especially its temporal trend in recently years, should be the first step. Beijing Cancer Registry (BCR) is a population-based cancer registry, which was set up to collect and manage cancer data of residents in Beijing. It fills the data gap of cancer incidence and prevalence in Beijing, and can be used to study the epidemiological distribution of cancer and survival patterns of cancer patients in Beijing temporally and spatially. In this article, we provide cancer incidence data of Beijing in 2014 overall by gender, age group, cancer site and geographical area.
Materials and methods
Data source
The BCR enrolls all cancer cases from secondary and tertiary hospitals in Beijing and the data of demography, diagnoses and survival are collected. It covers about 13 million residents in Beijing.
All cancer cases were further classified according to the International Statistical Classification of Disease and Related Health Problems 10th Revision (ICD-10) and International Classification of Disease for Oncology 2nd edition (ICD-O-2) (if it was not applicable for some cases with specific histological categorization, ICD-O-3 was used). The cancer data included in this paper were all malignant neoplasms, which were coded from C00-C96 under ICD-10. The rules for defining multiple primary cancer followed the International Rules for Multiple Primary Cancers (ICD-O Third Edition) (4). Benign brain and central nervous system tumors and in situ cancers were excluded from this analysis.
We used the rule from International Agency for Research on Cancer/International Association of Cancer Registries (IARC/IACR), which defines the date of admission to a hospital as the incidence date. All incidence dates from 1st January 2014 to 31st December 2014 were included in this analysis and were used to calculate incidence rate of cancers in 2014. The database only includes permanent residents in Beijing. Urban areas include 6 districts, which are Dongcheng, Xicheng, Chaoyang, Haidian, Fengtai and Shijingshan District. The rest 10 districts are categorized as rural areas, which are Mentougou, Fangshan, Daxing, Huairou, Shunyi, Changping, Pinggu, Tongzhou, Yanqing and Miyun District.
Information of population composition by the sex and age groups in 2014 was provided by the Beijing Municipal Bureau of Public Security.
Quality control
The data of new cancer cases were collected from the Health Information System of hospitals online passively, and re-abstracted actively. In each hospital, 1–2 part-time registrars were employed and trained to help collect data. All original data were checked by the BCR and the data quality was further evaluated by the percentage of morphology verification (MV) (%), the percentage of death certificate-only (DCO) (%) and the mortality to incidence ratio (M/I) based on the quality standard developed and described in the Chinese Guideline for Cancer Registration and the quality standard of “Cancer Incidence in Five Continents Volume IX” by IARC/IACR (5,6).
Statistical analysis
The cancer incidence rate was calculated in strata by sex, age group and area (urban and rural). The population composition of China in 1982 and Segi’s population structure (7) were used to calculate China and world age-standardized rate respectively [the age-standardized incidence rate by Chinese standard population (ASIRC) and by world standard population (ASIRW)]. The cumulative risk of developing cancer before 75 years old was calculated as the sum of age-specific incidences multiplied the interval between each two age groups. The annual percentage change (APC) in incidence rate was calculated by Joinpoint Regression Program (8) for the top ten common cancer types by sex. Data quality checking, evaluation and calculation were done with the IARC/IACR Cancer Registry Tools 2.05 (9) and Microsoft Excel 2016.
Results
Data quality
The overall data quality indicators, including MV%, DCO% and M/I, were 72.15%, 0.94% and 0.54, respectively. For males, they were 66.98%, 1.15% and 0.64, respectively, while for females, 77.40%, 0.74% and 0.44, respectively. For urban areas, they were 73.71%, 1.10% and 0.53, respectively, and for rural areas, 69.04%, 0.65% and 0.57, respectively.
Incidence
The cancer incidence in Beijing in 2014 by sex and area is shown in Table 1. Briefly, there were 45,300 newly diagnosed cancer cases in 2014 in Beijing, equivalent of about 5 newly diagnosed cancer patients every hour. The crude incidence rate of all cancer combined was 341.92/100,000 (343.50/100,000 for males and 340.33/100,000 for females). The ASIRC in 1982 was 143.48/100,000 (139.28/100,000 for males and 149.02/100,000 for females). The ASIRW was 182.99/100,000 (181.13/100,000 for males and 186.66/100,000 for females). The crude incidence rate, ASIRC and ASIRW were all higher in urban area than in rural area. However, after age standardization (ASIRC or ASIRW), the incidence rate for males in rural area is higher than that in urban area. The cumulative incidence rate for cancer before 75 years was 20.61%.

Full table
Age-specific incidence rate
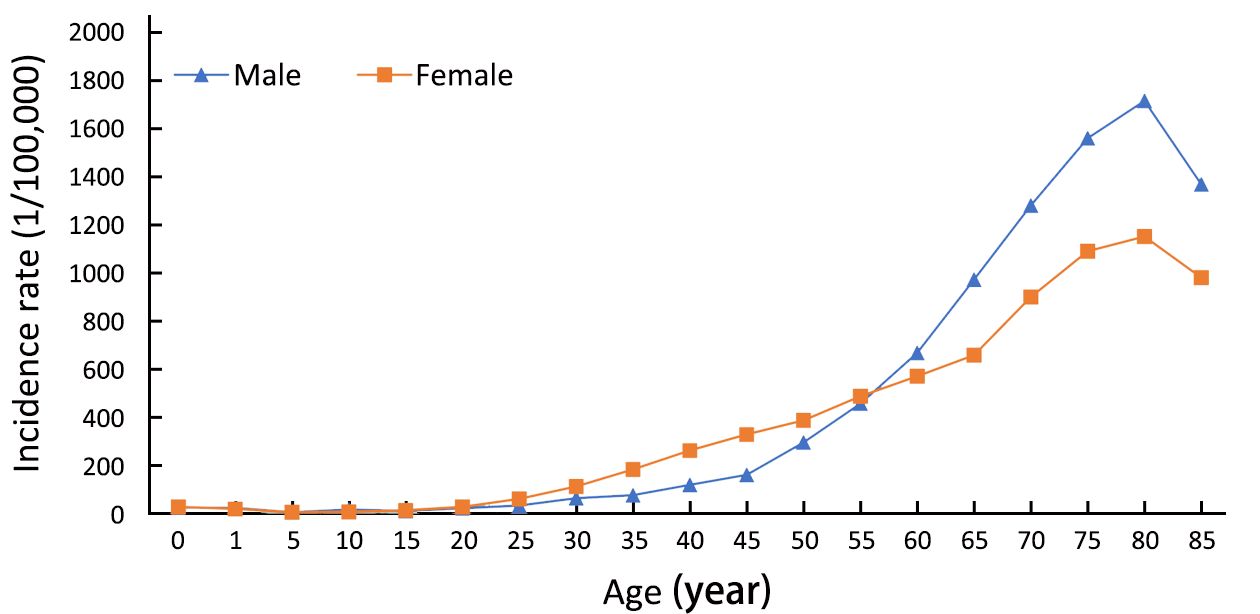
The age-specific incidence rate for Beijing in 2014 by sex is shown in Figure 1. The age-specific incidence rate was relatively low before 25 years old, while then increased significantly to the peak at the age group of 80–84 years. The pattern of age-specific incidence rate was similar in males and females. However, in the groups aged 15–59 years, the age-specific incidence rate was higher in females than in males for total cancer, while the pattern for males and females was opposite in the groups aged over 60 years old.
Top ten leading cancer types for the new cancer cases
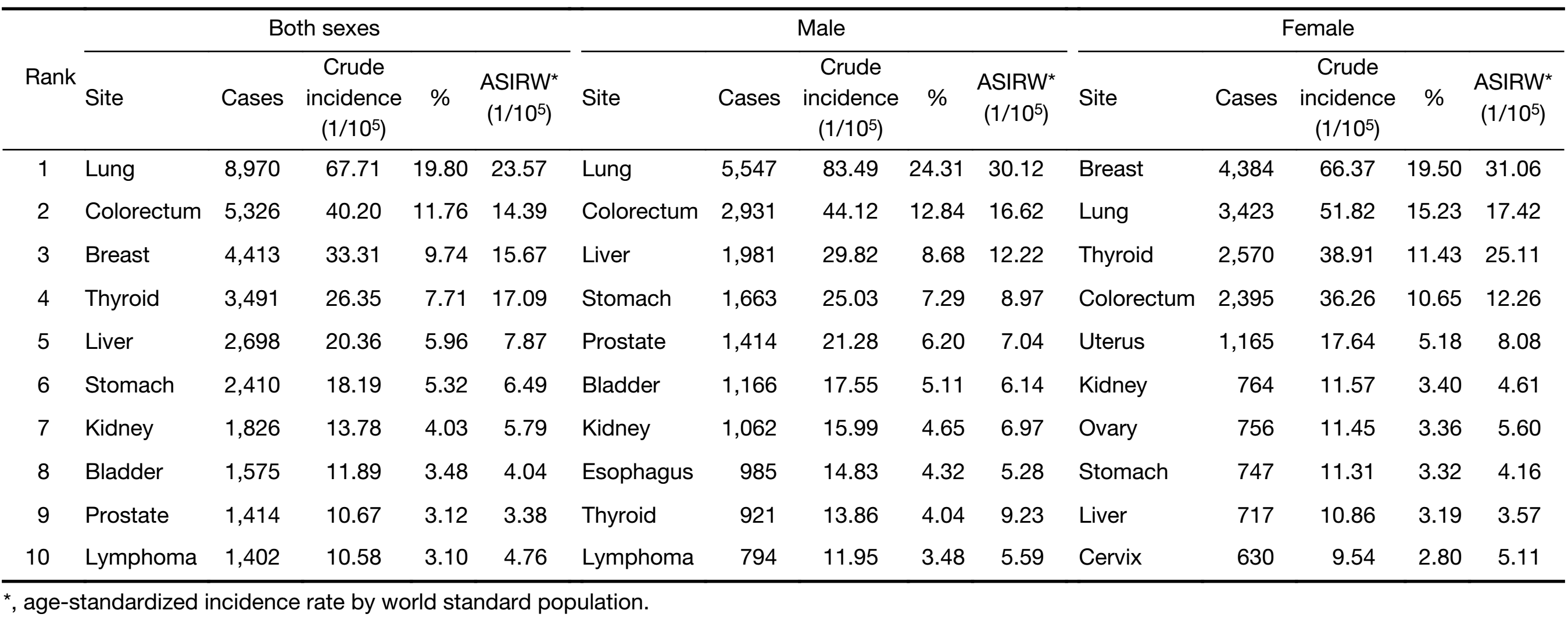
The top ten cancer types and their incidence rates overall and by sex and area are shown in Table 2–4. Lung cancer was the most common cancer type in Beijing in 2014, and 1 in 5 newly diagnosed cancer patients is lung cancer. The number of new cases and incidence rate for lung cancer is 8,970 and 23.57/100,000. It was followed by colorectal cancer, breast cancer, thyroid cancer and liver cancer with the numbers of new cancer cases were 5,326, 4,413, 3,491 and 2,698, respectively and with ASIRW were 14.39, 15.67, 17.09 and 7.87 per 100,000 people, respectively. The top ten cancer types accounted for 74.02% of all newly diagnosed cancer patients. Lung cancer is the most common cancer in males too, accounting for 24.31% of all newly diagnosed cancer patients, followed by colorectal cancer, liver cancer, stomach cancer and prostate cancer. Female most common cancer is breast cancer, accounting for 19.50% of newly diagnosed cancer cases and followed by lung cancer, thyroid cancer, colorectal cancer and uterus cancer.
Full table
Full table
Full table
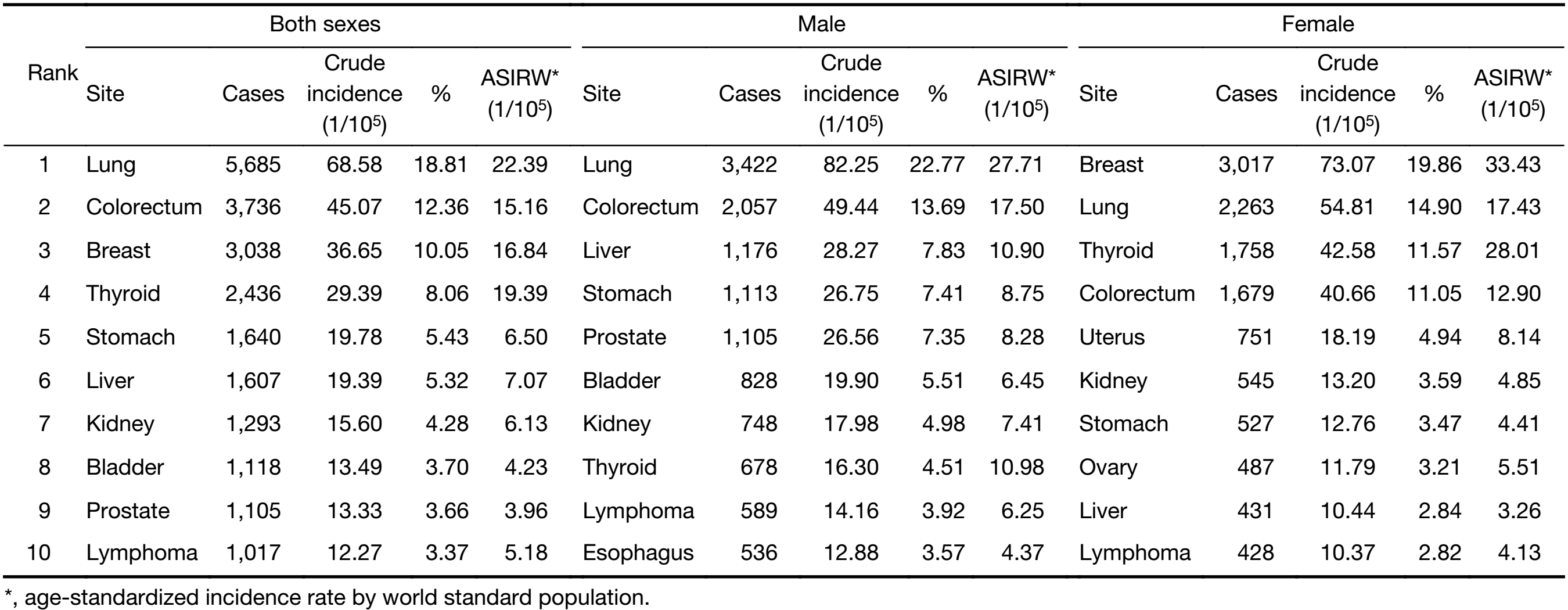
In urban area, lung cancer was the most common cancer type, followed by colorectal cancer, breast cancer, thyroid cancer and stomach cancer with new cancer cases of 5,685, 3,736, 3,038, 2,436 and 1,640, respectively and with ASIRW of 22.39, 15.16, 16.84, 19.39 and 6.50 per 100,000 people, respectively. The top five common cancer types for males in urban areas are lung cancer, colorectal cancer, liver cancer, stomach cancer and prostate cancer, while breast cancer, lung cancer, thyroid cancer, colorectal cancer and uterus cancer are the top five common cancer types for females in urban area.
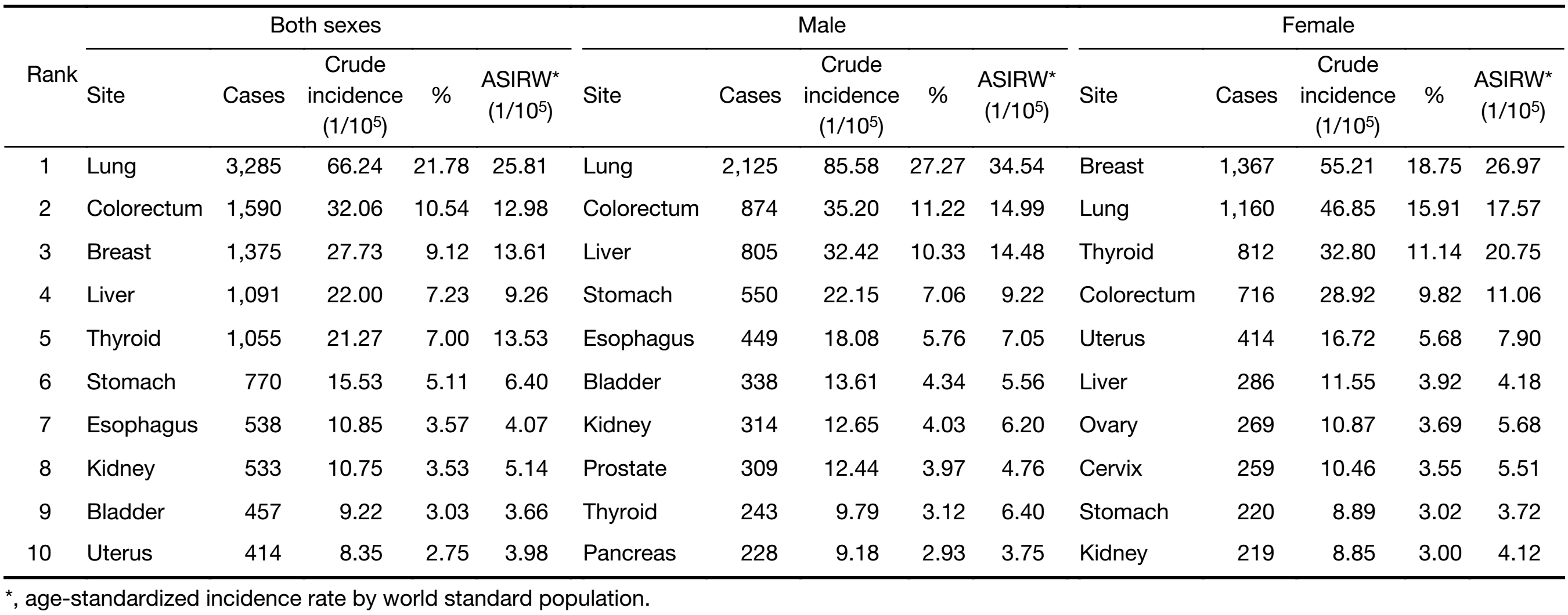
In rural area, lung cancer was the most frequently diagnosed cancer type too, followed by colorectal cancer, breast cancer, liver cancer and thyroid cancer with new cancer cases of 3,285, 1,590, 1,375, 1,091 and 1,055, respectively and with ASIRW of 25.81, 12.98, 13.61, 9.26 and 13.53 per 100,000 people, respectively. The top five common cancer types for males in urban areas are lung cancer, colorectal cancer, liver cancer, stomach cancer and esophageal cancer, while breast cancer, lung cancer, thyroid cancer, colorectal cancer and uterus cancer are the top five common cancer types for females in rural area.
Trends in top ten cancer types
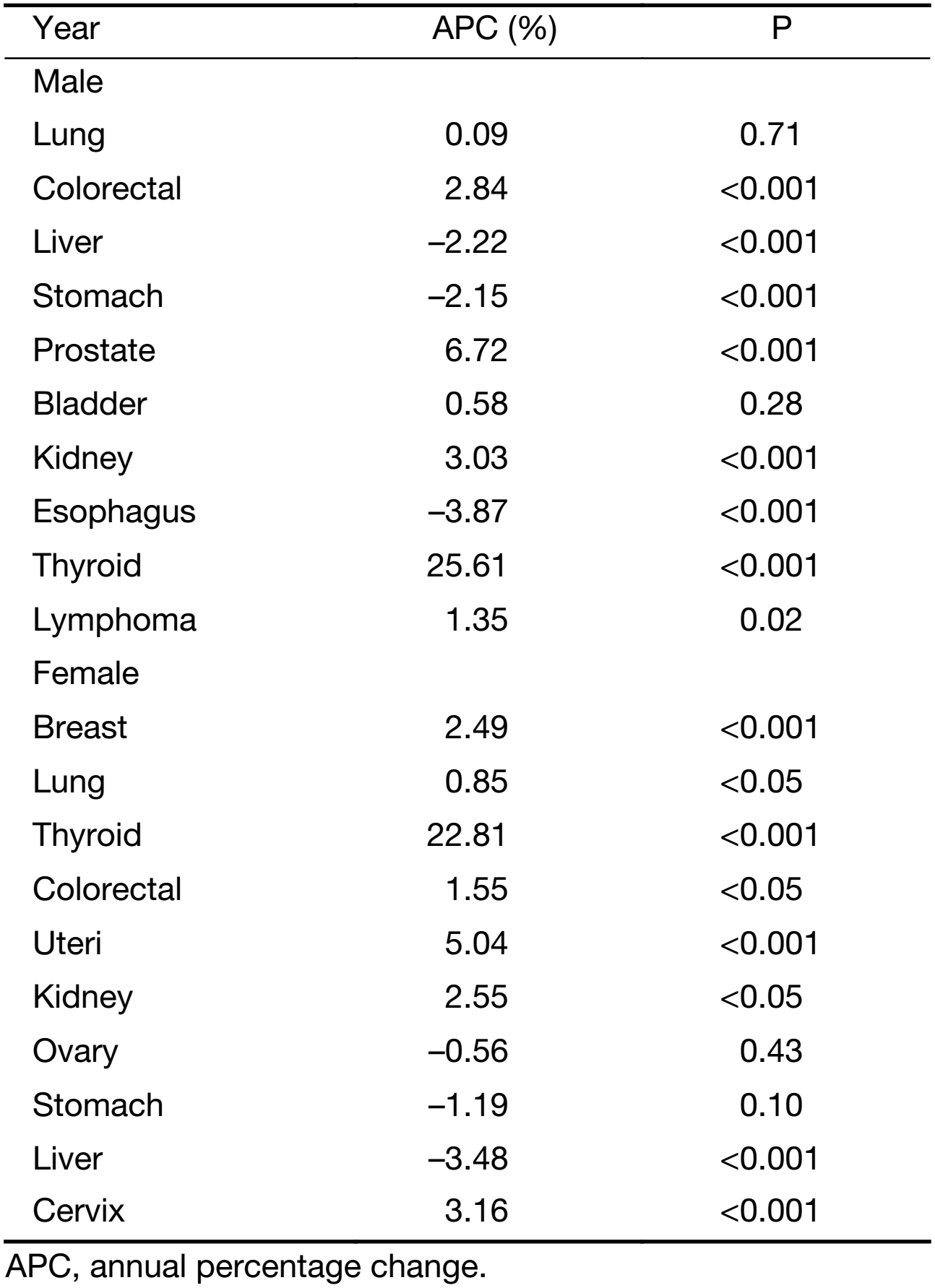
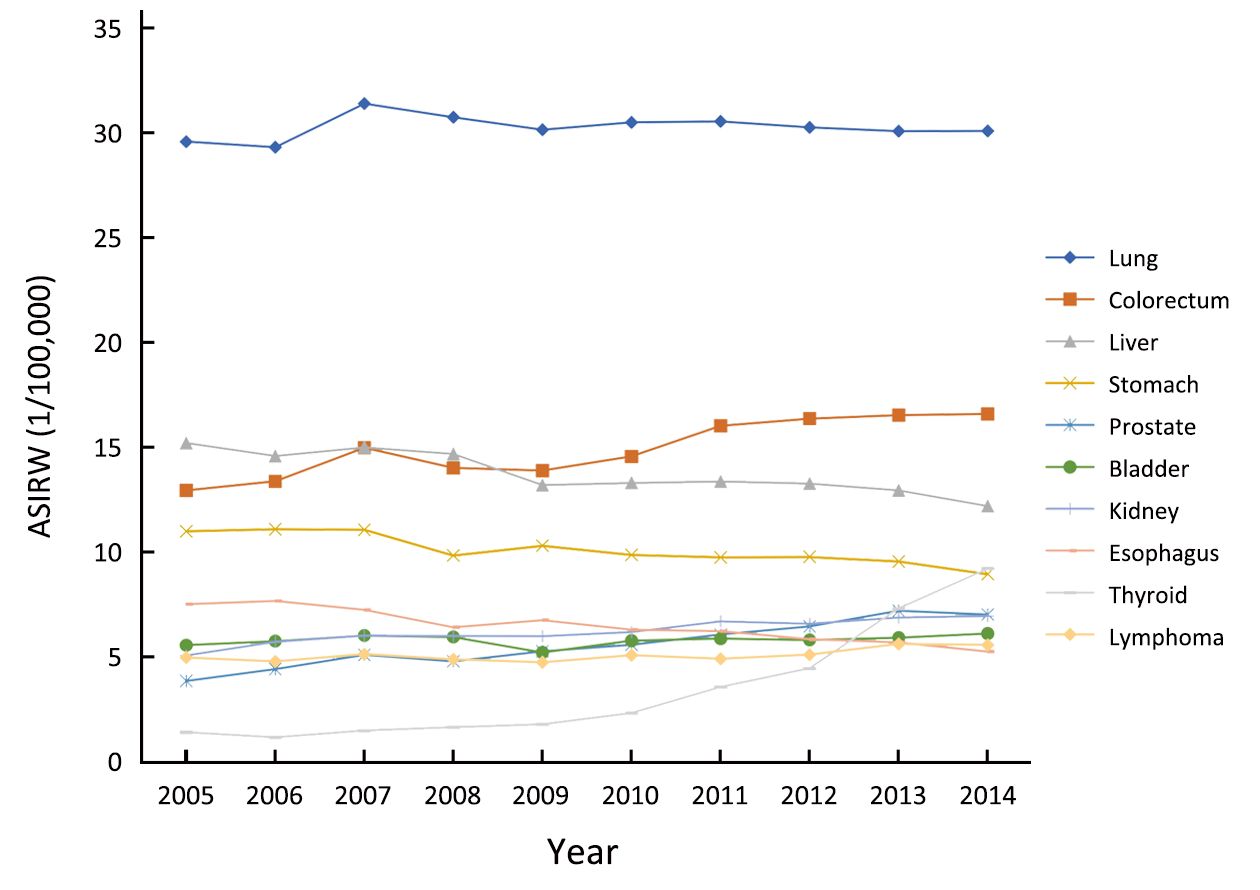
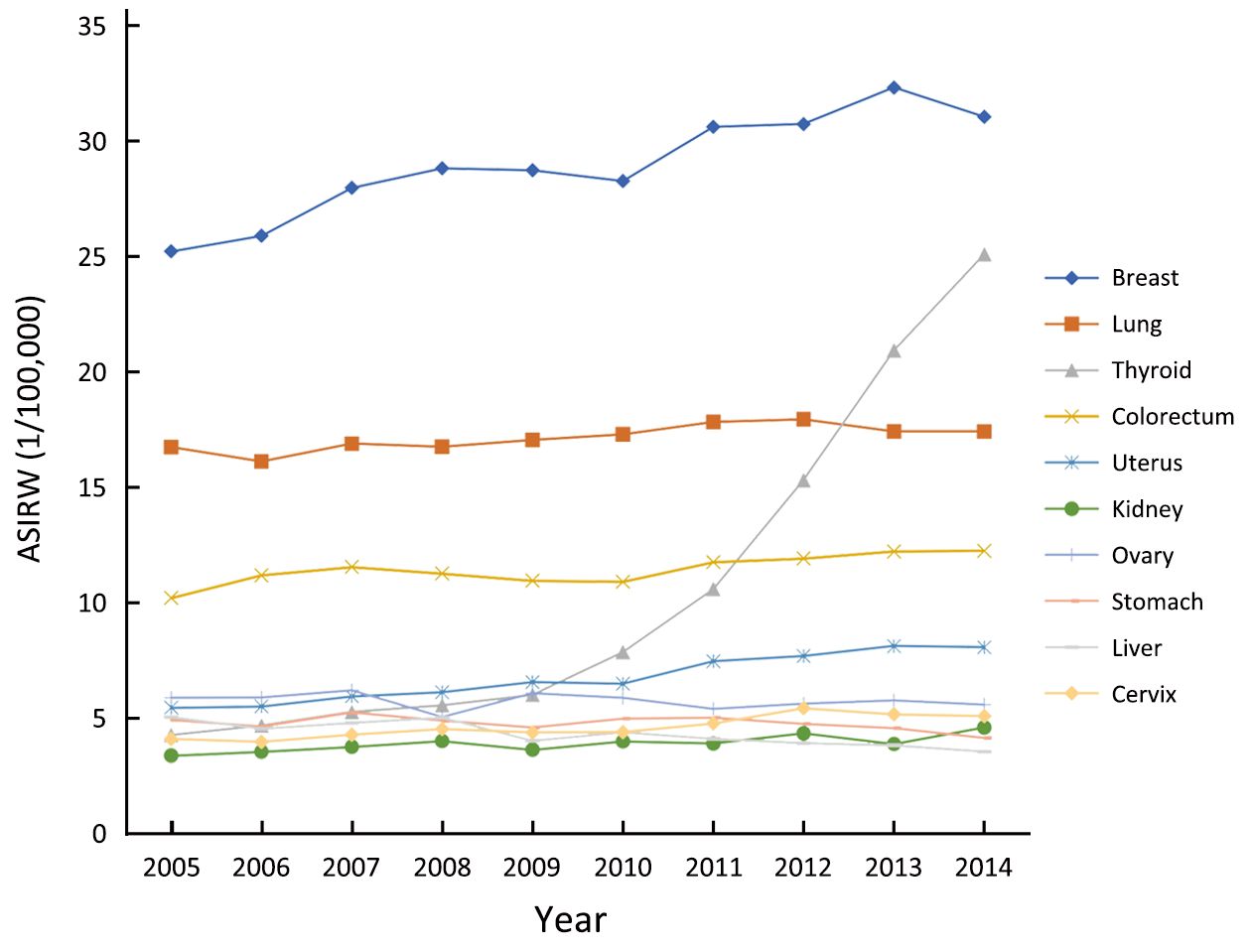
The trends of top ten cancer types in Beijing between 2005 and 2014 by sex are illustrated in Table 5, Figure 2 and Figure 3. Decreased trends for liver cancer were observed in males and females, with the APC of –2.22% and –3.48% respectively. The incidence rate of esophageal cancer also decreased significantly in the last ten years for males and the APC was –3.87%. The incidence rate of thyroid cancer showed a significant increase for both sex groups, the APC for males and females were 25.61% and 22.81%, respectively. Additionally, incidence rates of both colorectal cancer and kidney cancer slightly increased for both sex between 2005 and 2014. However, the incidence rate for lung cancer was relatively stable for males, and slightly increased for females with the APC of only 0.85% for the past decade. The incidence rates of prostate cancer increased approximately 6.72% per year and around 2.15% reduction of incidence rate per year for stomach cancer was observed for males. The incidence rates for lymphoma and bladder cancer were stable between 2005 and 2014. For females, incidence rate for breast cancer, uterus cancer and cervix cancer increased, while the incidence rate for ovary cancer and stomach cancer was relative stable over the past ten years.
Full table
Discussion
BCR is a population-based cancer registry which is aiming to understand the epidemiologic pattern of cancer and improve cancer prevention in Beijing areas. High quality cancer statistics generated from cancer surveillance system could help the policy-makers, researchers and oncology clinicians to understand the huge burden of disease from cancer and its temporal and spatial variations, and finally develop effective strategy to prevent cancers.
In 2014, 144 secondary and tertiary hospitals reported new cancer cases to BCR. There were 45,300 newly diagnosed cancer cases in Beijing in 2014. And the crude incidence rate and ASIRW are 341.92/100,000 and 182.99/100,000, respectively. Compared to other high urbanized area in China, the ASIRW was slightly lower in Beijing in 2014 (10).
Epidemiologic pattern of cancer in Beijing was different from national pattern of China, though lung and breast cancer are both leading cancer types for males and females in Beijing and overall China. However, incidence rates of some digestive system cancer, such as liver, esophagus and stomach cancer in China are 2–4 folds higher compared to Beijing areas, while incidence rates of prostate cancer for males and breast cancer for females in Beijing areas are higher than national incidence rates of China. The ASIRW for thyroid cancer in Beijing was more than two times compared with national data. In addition, urinary system cancers in Beijing areas were more prevalent than overall China, for example, the renal cancer is the top ten cancers in both sex groups in Beijing in 2014 and bladder cancer incidence rate for males in Beijing was higher than that in other areas. For female genital caner, the incidence rate of cervix cancer in Beijing was lower than that of general population in China, however, for uterus and ovary cancer, it was higher in Beijing (11,12).
The ASIRW of liver cancer in Beijing was less than half of national incidence rate and has been kept decreasing for the last decade (12). Hepatics B infection has been proven to be the most important risk factor of primary liver cancer. Three sero-epidemiological studies of hepatitis B prevalence among general population in Beijing were conducted in 1992, 2006 and 2014, respectively, and it found that the age standardized HBsAg sero-positive rate dropped from 6.01% in 1992 to 3.02% in 2006 and 2.73% in 2014 (13,14), which was attributed to planned immunization. And it is considerably lower in Beijing than in the national level, which were 9.75% in 1992 and 7.18% in 2006 and it may result in differences in liver cancer incidence (13,14).
The ASIRW was higher in urban areas than in rural area and this is consistent with pattern identified in national studies (12). Comparing patterns in urban and rural areas in Beijing, incidence of liver cancer and lung cancer was higher in rural area than in urban area for both sex groups. Besides, incidence of esophagus cancer and stomach cancer was higher in rural area for males in Beijing compared to urban area.
The ASIRW for all cancers in females was higher than that in males in Beijing. The urban areas shared the same pattern, while it was opposite in rural area. The incidence rates for most types of cancers increase with age. The age-specific cancer incidence rate is low for both females and males before 25 years old. Before 55 years old, the incidence for females is higher than that for males and after that age the pattern is opposite. One of the possible reasons for that is the age of diagnosis of cervix cancer and breast cancer for females is younger than other types of cancers, such as breast cancer for females, after 40 years old, the incidence rate increases fast. And after 55 years old, the cancer incidence rate for males has a rapid growth and becomes higher than that of females because of higher prevalence of cancer related risk factors, such as tobacco use and alcoholic beverage intake.
Tobacco smoking was classified into Group 1 carcinogens to humans by IARC. It has sufficient evidence about the relationship of smoking to a group of cancers, such as lung cancer, esophagus cancer and stomach cancer (15). Successful tobacco control initiatives have been proven to be effective for reducing cancer incidence. According to the result of a survey, smoking rate of 15+ adults in Beijing has been decreased from 34.5% in 1997 to 28.0% in 2001 and 26.9% in 2004 (16) and approximately 23% in recently years after three smoking cessation rules implemented in Beijing in 1996, 2008 and 2015. The effective tobacco control may contribute considerably to the decreased incidence rates for esophagus cancer, stomach cancer and the plateau status of lung cancer incidence rate in the last decade. Though the smoking rate in Beijing is slightly lower than that in national level (24%) (12), it is still quite higher than that in developed countries, such as the United State (15.1%) (17). Thereby, intensified efforts are still needed for tobacco control.
Besides smoking control, other effective lifestyle interventions on reducing consumption levels of alcoholic beverages and very hot beverage, pickled vegetables and processed meat along with controlled infection of helicobacter pylori could lead to decreased incidence rates of esophagus and stomach cancer.
With the westernized lifestyles and rapid urbanization, the pattern of cancer incidence in Beijing is becoming more closed to western countries in recent years. For example, the ascending trend of incidence rates of colorectal cancer and breast cancer observed in Beijing is similar to western countries. These may be partly due to higher fat, lower fiber intake and increased sedentary behaviors.
The incidence of thyroid cancer has the fastest growth in both females and males for the last decade and it has already become the third most common cancer for females and ninth for males. This rapid growth was also discovered in other provinces of China, especially in urban area (18-22). However, the mortality rate for thyroid cancer was stable (11,12,23). The possible reasons include widespread use of the modern imaging technologies and fine-needle aspiration biopsy or cytology in thyroid cancer detection and sensitivity improvement of inspection equipment, such as neck ultrasound, which allow more micro carcinoma were detected than before. Additionally, with the improvement of health consciousness, more and more people choose to participate in the annual health check including examination of neck ultrasound. But on the other hand, some researchers believed that personal exposure to risk factor also leads to the increasing for the incidence of thyroid cancer, including radiation exposure, diet, obesity and other life style factors. All of these contributors need to be taken into account to strategy development for thyroid cancer related prevention and control. We need to find the balance between over-diagnosis and effective management of thyroid cancer (23,24).
Cancer screening program may influence the cancer incidence too. Cervical and breast cancer screening program for female residents aged 35–64 years was implemented in Beijing since 2009. That maybe contributes to the slight increasing for those two cancers. Subsequently in 2012, two more cancer screening programs were launched in Beijing for five most common cancers including liver, upper digest tract, colorectum, breast and lung cancer. However, it is limited to small sample size and duration of time, and it is hard to identify the influence on cancer incidence at present. Additionally, the HPV vaccine has been approved in Beijing and used in general practice at the end of 2017, which might also have an effect on incidence of cervix and other genital system cancers in the future.
Rapid aging and population growth along with age-specific incidence increasing will still lead to rising disease burden of cancer in the foreseeable future. To address this issue, the government should assure cancer patients can get access to optimal health care, at the meantime, risk factor oriented intervention and early detection of cancer for high risk population should be strengthened.
Acknowledgements
We acknowledged the cooperation of all the hospitals in providing cancer incidence data. This study was support by the Beijing Young Talent Program (No. 2016000021469G189).
Footnote
Conflicts of Interest: The authors have no conflicts of interest to declare.
References
- National Bureau of Statistics of China. China Statistical Yearbook, 2010. Beijing: China Statistics Press, 2010.
- Ferlay J, Soerjomataram I, Ervik M, et al. GLOBOCAN 2012, Cancer Incidence and Mortality Worldwide: IARC CancerBase No. 11; Lyon; IARC. 2013. Available online: http://globocan.iarc.fr
- People’s Government of Beijing Municipality. Beijing Hygiene and Population Health Report, 2014. Beijing: People’s Medical Publishing House, 2015.
-
IARC, WHO, IACR, ENCR. International rules for multiple primary cancers (ICD-O Third Edition). Lyon, France: International Agency for Research on Cancer, 2004. Available online: http://www.iacr.com.fr/
images/doc/MPrules_july2004.pdf - Curado MP, Edwards B, Shin HR, et al. Cancer Incidence in Five Continents. Vol. IX. Lyon: IARC, 2008:1-837.
- National Cancer Center. Chinese guideline for cancer registration. Beijing: People’s Medical Publishing House, 2016.
- Ahmad OB, Boschi-pinto C, Lopez AD, et al. Age standardization of rates: a new WHO standard. GPE Discuss Pap Ser 2001;(31):1-14. Available online: http://www.who.int/healthinfo/paper31.pdf
- Joinpoint Regression Program, Version 3.4.3, 2017. Statistical Methodology and Applications Branch, Surveillance Research Program, National Cancer Institute.
-
Ferlay J. The IARCcrgTools Programs. Lyon: IARC, 2006. Available online: http://www.iacr.com.fr/index.
php?option=com_content&view=category&layout=blog&id=68&Itemid=445 - Fei FR, Hu RY, Zhong JM, et al. Morbidity and mortality of malignant tumor in Zhejiang province, 2014. Zhonghua Liu Xing Bing Xue Za Zhi (in Chinese) 2016;37:694–8. DOI:10.3760/cma.j.issn.0254-6450.2016.05.022
- Chen W, Zheng R, Zhang S, et al. Cancer incidence and mortality in China in 2013: an analysis based on urbanization level. Chin J Cancer Res 2017;29:1–10. [PubMed] DOI:10.21147/j.issn.1000-9604.2017.01.01
- Chen W, Zheng R, Zhang S, et al. Cancer incidence and mortality in China, 2013. Cancer Lett 2017;401:63–71. [PubMed] DOI:10.1016/j.canlet.2017.04.024
- Wu J, Zhang W, Han L, et al. A sero-epidemiological study on hepatitis B among general population in Beijing. Zhonghua Liu Xing Bing Xue Za Zhi (in Chinese) 2007;28:555–7.
- Gao P, Wang H, Chen WX, et al. A sero-epidemiological study of hepatitis B among general population in Beijing. Zhonghua Liu Xing Bing Xue Za Zhi (in Chinese) 2016;37:658–62. DOI:10.3760/cma.j.issn.0254-6450.2016.05.014
- Cogliano VJ, Baan R, Straif K, et al. Preventable exposures associated with human cancers. J Natl Cancer Inst 2010;103:1827–39. [PubMed] DOI:10.1093/jnci/djr483
- Li C, Cui X, Rao Y, et al. Study on the rates of smoking among the residents of Beijing, from 1997 to 2004. Zhonghua Liu Xing Bing Xue Za Zhi (in Chinese) 2007;28:453–6.
- Jamal A, King BA, Neff LJ, et al. Current cigarette smoking among adults — United States, 2005-2015. MMWR Morb Mortal Wkly Rep 2016;65:1205–11. [PubMed] DOI:10.15585/mmwr.mm6544a2
- Mu H, Li Y, Zhang R, et al. Trend of incidence and mortality of thyroid cancer in five cities in Liaoning Province, 2000-2011. Zhongguo Zhong Liu (in Chinese) 2015;24:889–95. DOI:10.11735/j.issn.1004-0242.2015.11.A001
- Xiang F, Huang F, Zhang YY, et al. Trend in incidence of thyroid cancer in Jiading district of Shanghai, 2003-2013. Zhonghua Yu Fang Yi Xue Za Zhi (in Chinese) 2016;50:656–8. DOI:10.3760/cma.j.issn.0253-9624.2016.07.018
- Li K, Lin G, Zhou Q, et al. Time trends of the incidence of thyroid cancer in urban Guangzhou, 2000-2011. Zhonghua Yu Fang Yi Xue Za Zhi (in Chinese) 2015;49:142–6. DOI:10.3760/cma.j.issn.0253-9624.2015.02.009
- Liang D, Li D, Shi J, et al. Epidemic trends of thyroid cancer in Hebei Province, 2010-2013. Zhongguo Zhong Liu (in Chinese) 2016;25:973–8. DOI:10.11735/j.issn.1004-0242.2016.12.A006
- Sun J, Xu X, Cai Q, et al. Epidemiological study on thyroid cancer in China. Zhongguo Zhong Liu (in Chinese) 2013;22:690–3. DOI:10.11735/j.issn.1004-0242.2013.09.A002
- Yang L, Wang N. Progress of Epidemiology in thyroid Cancer. Zhonghua Yu Fang Yi Xue Za Zhi (in Chinese) 2014;48:744–8. DOI:10.3760/cma.j.issn.0253-9624.2014.08.021
- Liu S, Zhang X. Epidemiology and management guidelines of thyroid cancer. Zhonghua Er Bi Yan Hou Tou Jing Wai Ke Za Zhi (in Chinese) 2016;51:146–9. DOI:10.3760/cma.j.issn.1673-0860.2016.02.021