
Feasibility of differentiating T3 from T4a gastric cancer in different Lauren classification by determining serosa invasion: Diagnostic performance of high enhanced serosa sign
Introduction
Gastric cancer is one of the leading causes of cancer death worldwide, which is particularly common in eastern Asia (1). Tumor invasion and lymph node metastasis are two important prognostic factors of gastric cancer. Conventional fiberoptic endoscopy and upper gastrointestinal series have been used as first line procedures for the early detection of gastric cancer. Although these methods can discriminate between early gastric cancer (EGC) and advanced gastric cancer (AGC) to some degree (2), they cannot provide sufficient information regarding the transmural invasion of tumor. Given the growing popularity of less-invasive therapeutic options such as endoscopic mucosal resection, endoscopic submucosal dissection and laparoscopy-assisted gastric resection, accurate preoperative staging is particularly important for alternative treatment strategies and prognostic evaluations (3,4).
In the eighth TNM staging system of the American Joint Committee on Cancer/International Union Against Cancer (AJCC/UICC) released in 2016, the T categories for gastric cancer is the same as it was defined in the seventh TNM staging system (5,6). T1 tumor have been divided into T1a (lamina propria or muscularis mucosae) and T1b (submucosa), T2 is defined as a tumor invading the muscularis propria, T3 is defined as a tumor invading the subserosal connective tissues and T4 is defined as a tumor invading the serosa (T4a) or adjacent structures (T4b).
The assessment of serosa invasion before the surgery has a crucial significance because for locally AGC with serosal invasion, neoadjuvant chemotherapy is being used more frequently to downstage the tumor and treat micrometastases (7,8). Moreover, differentiation between T3 and T4a gastric carcinoma is very important to determine the appropriate procedure of surgery and expect the prognosis, especially for the risk of peritoneal dissemination. For T4a gastric cancer staging, the reported computed tomography (CT) accuracy varies considerably, ranging from 77.8% to 93.5% (6-8). The reported CT criteria for T4a gastric cancer are extraluminal extension of the gastric wall and haziness of the perigastric fat (8). The paragastric inflammatory strands may mimic the cancer infiltration out of the serosa and lead to the overstaging of T3 tumors during the preoperative staging of gastric cancers. A previous study founded that the high density outer layer of the gastric wall might be associated with cancer involvement of the serosa, and refered to this sign as hyperattenuating serosa sign, which was assumed to indicate a poor prognosis (9).
Lauren classification is also reported to be a factor associated with the prognosis, which is one of the most commonly used pathological classification systems of gastric adenocarcinoma (10,11). This system classifies gastric adenocarcinoma into the intestinal, diffuse, or mixed types on the basis of histology. Each type has a distinct pathology, epidemiology, and prognosis (10-14). The intestinal-type is known to have a higher survival rate than the diffuse-type (11). Gastric cancers may thus show diverse enhancement patterns on contrast-enhanced CT.
The purpose of our study was to further evaluate the clinical value of the high enhanced serosa sign on CT in determining the serosa invasion in patients with different Lauren types of gastric cancers.
Materials and methods
This retrospective study was approved by the Institutional Review Board of Peking University Cancer Hospital, and the requirement of informed consent was waived.
Patients
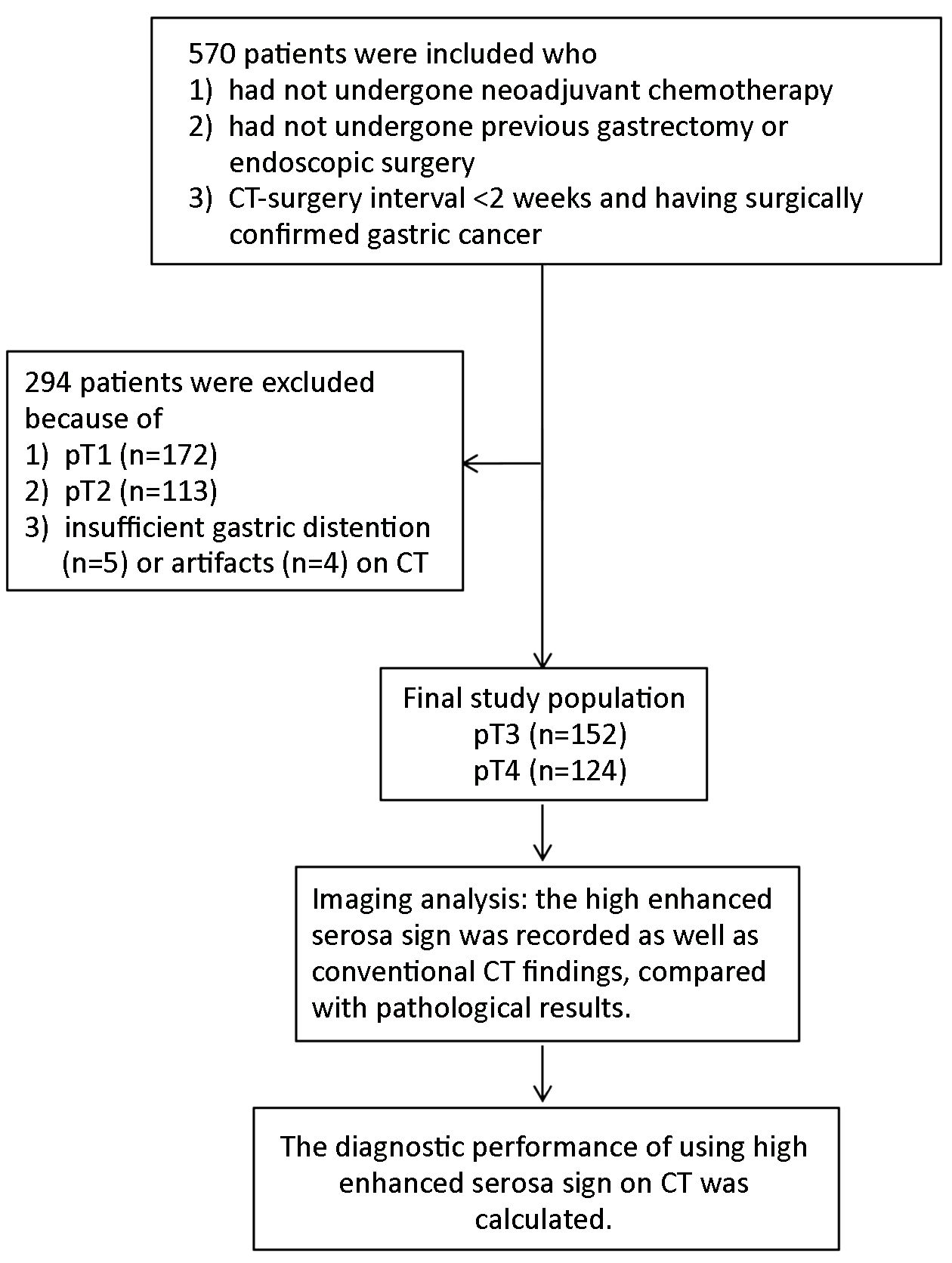
Between January 2012 and December 2015, 570 consecutive patients who underwent both preoperative contrast enhanced CT scan and gastrectomy in Peking University Cancer Hospital were retrospectively enrolled in this study according to the following inclusion criteria. Patients were enrolled who: 1) had not undergone neoadjuvant chemotherapy; 2) had not undergone previous gastrectomy or endoscopic surgery; and 3) had undergone gastrectomy within 2 weeks after preoperative CT. Two hundred and ninety-four patients were excluded because 1) pathologically proven pT1 or pT2 gastric cancers (n=285); or 2) CT images with poor distention (n=5) or artifacts (n=4). Finally, 276 patients (159 males, mean age 58.3±9.4 years and 117 females, mean age 61.7±11.8 years) were included in this study (Figure 1).
CT protocol
Multi-detector row was performed using a 64-detector row CT scanner (LightSpeed 64; GE Healthcare, Milwaukee, Wisconsin, USA). Each patient had been fasting for more than 6 h prior to the CT examination. To reduce gastric motility and enable gastric distention, the patients were given an intramuscular injection of 10 mg anisodamine 10–15 min before the examination and received 8 g gas-producing crystals orally with 10 mL of water orally shortly before CT scanning. Upper abdominal unenhanced CT scans from the diaphragmatic domes to 2 cm below the lower margin of the air-distended gastric body were acquired. Subsequently, a total of 100 mL of non-ionic contrast medium (Ultravist; Schering, Berlin, Germany) was administered intravenously through an 18-gauge angiographic catheter inserted into an antecubital vein at 3 mL/s by using an automatic injector. Contrast-enhanced CT scans were performed in the arterial phase (start delay, 30 s), in the portal venous phase (70 s). Unenhanced scan was also required for all patients. The CT parameters used were as follows: collimation of 0.625 mm, gantry rotation time of 0.5 second, tube voltage of 120–140 kVp, tube current-time product of 300–350 mAs, and table feed per rotation of 15 mm. Using these raw data sets, both the arterial and portal venous phase axial CT images were reconstructed with a 5 mm section thickness and a 5 mm reconstruction interval for clinical interpretation. To further analyze the status of serosa invasion, multiplanar reconstruction (MPR) images were done with section thickness of 0.625 mm.
Image analysis
Two abdominal radiologists (with 5 and 15 years of experience, respectively, in abdominal CT, as well as 4 and 8 years of experience in three-dimensional MPR approaches and interpretation performed the image analysis. They were blinded to clinical and pathological data and independently evaluated CT images at the workstation before surgery by using transverse CT (5 mm) and MPR images (0.625 mm or greater) with soft-tissue window settings. Differences in assessment were evaluated by kappa coefficient analysis.
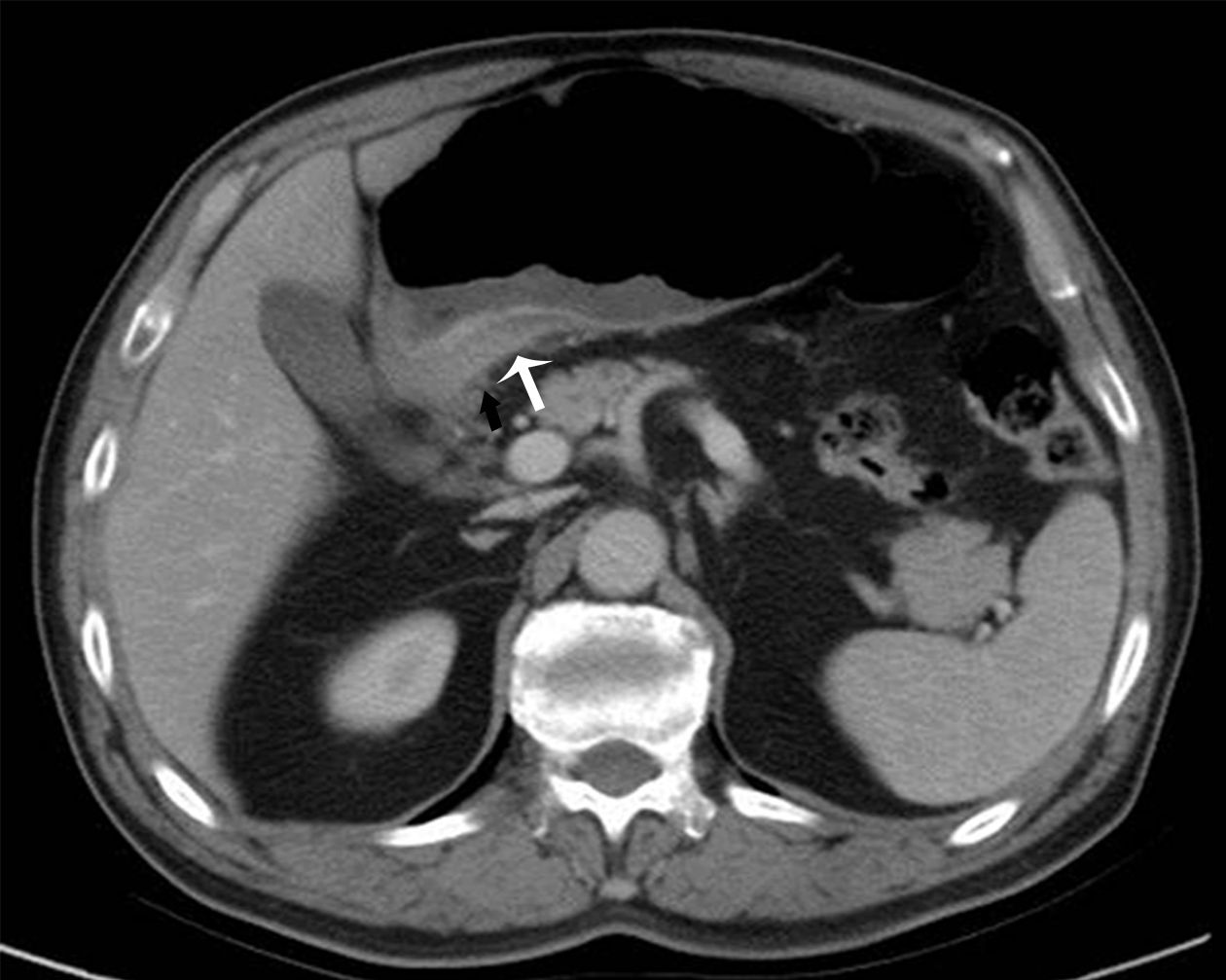
We defined the serosa involvement criteria based on the paper written by Kim et al (9). In that paper, the association between the high density outer layer of the gastric wall and the involvement of the serosa was hypothesized and defined as hyperattenuating serosa sign. The high enhanced serosa sign on CT was defined as a focal or diffuse thickened hyperattenuating outer layer of the gastric wall. We concluded the standards of the evaluation of the high enhanced serosa as follows: 1) It was calculated when it was seen in either the arterial or portal phase; 2) The gastric layers could be stratified by the attenuation value. As in Figure 2, the high enhanced serosa located in the outer layer of the gastric wall (white arrow) can be differentiated clearly from the inner hypoattenuating layer; and 3) The high enhanced serosa was evaluated in the largest tumor section on transverse or coronal or sagittal images using MPR.
The high enhanced serosa sign was the only criteria we use to evaluate the serosa involvement. Moreover, for all cancerous lesions, the following conventional CT features were recorded as well: the extraluminal extension, the blurring and obliteration of the fat plane. The extraluminal extension was defined as the irregular outer layer of the gastric wall. The blurring and obliteration of the fat plane was defined as linear or reticular structures in the fatty layer surrounding the cancerous lesion.
The efficacy of the discrimination of T3 from T4a in different Lauren types of gastric cancers by the high enhanced serosa sign on CT and the conventional CT features was calculated. The diagnostic accuracy was calculated by using surgical and histopathologic results as reference standards.
Pathological evaluation
The pathological features of gastric cancers were officially reported by a specialist with 10 years of experience in gastrointestinal pathology of Department of Pathology, Peking University Cancer Hospital. T-stage was determined using the pathological findings of surgical specimens as reference standards according to the eighth edition of the AJCC and the UICC TNM classification (5).
Intestinal or differentiated types include papillary and tubular adenocarcinomas. In intestinal tumors, tumor cells exhibit adhesion, and are arranged in tubular or glandular formations and are often associated with intestinal metaplasia (10,14). This type of gastric cancer is associated with lymphatic or vascular invasion, and the lesions are scattered in distant positions (15). By contrast, in diffuse gastric cancer, tumor cells lack adhesion and infiltrate the stroma as single cells or small subgroups, leading to a population of noncohesive, scattered tumor cells (11,12). Intracellular mucus may push the nucleus of the cell aside to form signet-ring cell carcinoma. Mixed-type shows a mixture of glandular and signet ring/poorly cohesive cellular histological components (16).
The locations of tumors were recorded as fundus, body and antrum. When the tumor occupied more than two areas, the larger region affected by the tumor was selected.
Statistical analysis
The demonstration of the high enhanced serosa seen on CT between T3 and T4a was compared with chi-square test, as well as the conventional CT findings. For each of the three Lauren types of gastric cancer, accuracy, sensitivity, specificity, positive predictive value (PPV), and negative predictive value (NPV) were calculated for the diagnosis of serosa invasion (pT4a stage) using the demonstration of the high enhanced serosa on CT. The difference in the judgement of serosa invasion between intestinal-type and diffuse-type was also tested with chi-square test. Multiple comparison was corrected by the Bonferroni method.
The agreement of judging hyperattenuating serosa sign between two raters was assessed using Kappa coefficient, 0–0.20, 0.21–0.40, 0.41–0.60, 0.61–0.80 and 0.81–1 indicated very poor, poor, moderate, substantial and excellent agreement, respectively.
All statistical analyses were performed using the IBM SPSS Statistics (Version 22.0; IBM Corp., New York, USA). P<0.05 was considered statistically significant.
Results
Pathological findings
In the 276 patients with AGC, T stages of gastric cancer of T3 and T4a were respectively found in 152 and 124 patients. The locations of gastric cancer included the fundus (n=96), body (n=93) and antrum (n=87). The histological types of gastric cancer included 89 intestinal-type, 86 diffuse-type and 101 mixed-type lesions.
Diagnosis performance using the high enhanced serosa sign
The two abdominal radiologists achieved substantial agreement, with Kappa coefficient of 0.63, P<0.001. The emergence rate of high enhanced serosa was significantly higher in T4a gastric cancer than in T3 gastric cancer in both two readers (P<0.001). The diagnosis performance of two radiologists using the high enhanced serosa sign on CT in determining the serosa invasion of patients of gastric cancers are shown inTable 1.

Full table
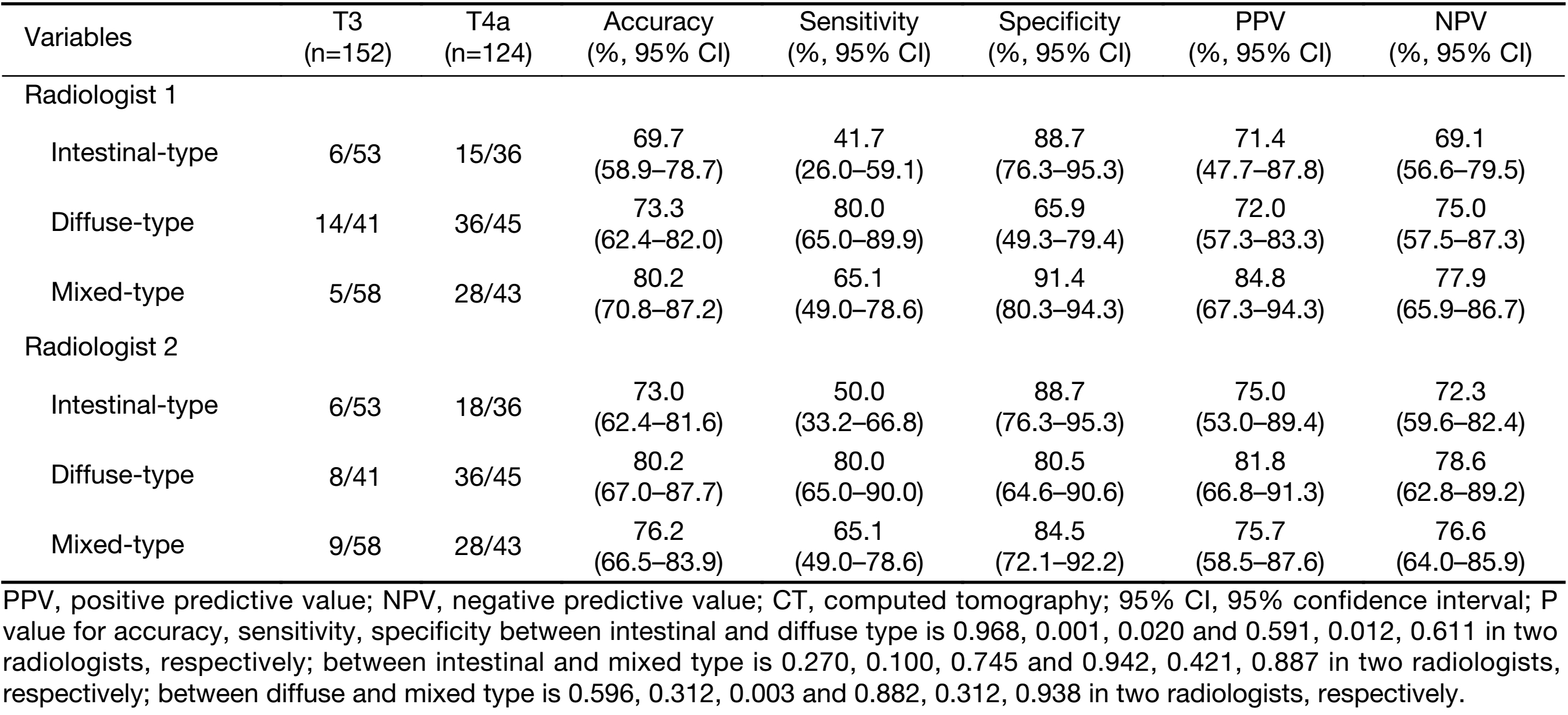
The judgement of serosa invasion with the highest sensitivity was in the diffuse-type (80.0%). The results indicated that, compared to the diffuse-type, the sensitivity of the judgement of serosa invasion using the high enhanced serosa seen on CT in intestinal-type was significant lower (the P-values of two radiologists were 0.001, 0.012, respectively), while the specificity of diagnosis was higher (the P-values of two radiologists were 0.020, 0.611, respectively). There is no significant difference in the accuracy of diagnosis between intestinal-type and diffuse-type of gastric cancers (the P-values of two radiologists were 0.968, 0.591, respectively). The specificity between the mixed-type and diffuse-type was significant different in one radiologist (the P-value was 0.003), while there was no significant difference between the mixed-type and intestinal-type. The accuracy, sensitivity, specificity, PPV and NPV of the high enhanced serosa sign on CT in determining the serosa invasion of patients with different Lauren types are shown in Table 2.
Full table
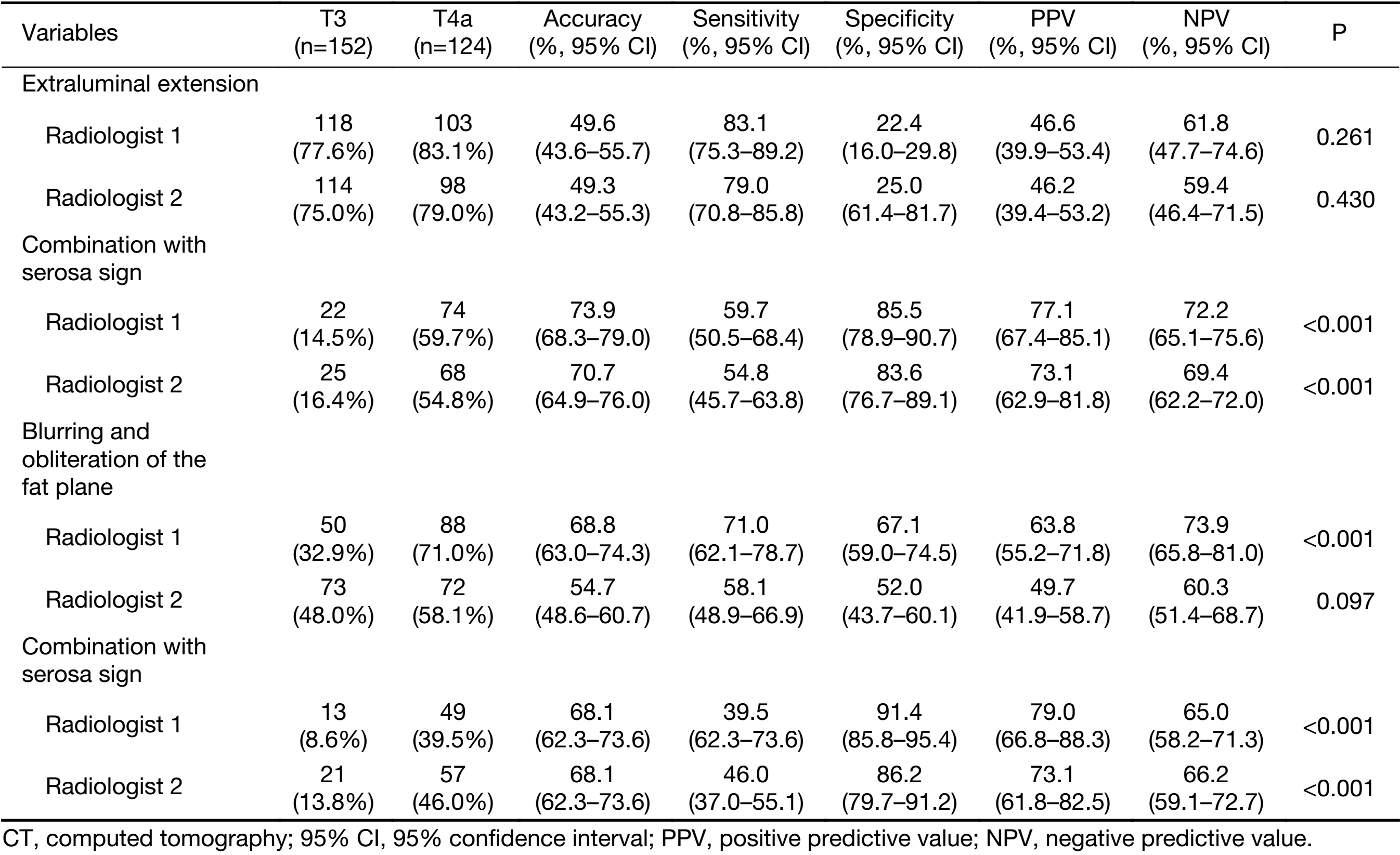
All CT findings were seen more often in T4a than in T3 gastric cancers, these conventional CT findings were not significantly different between T3 and T4a gastric cancer. The diagnostic performance of the conventional CT findings between patients with T3 and T4a gastric cancer are shown in Table 3. However, the combination of the high enhanced serosa sign with conventional CT signs shows significant difference between T3 and T4a gastric cancers. The diagnostic accuracy was increased in both radiologists after the combination.
Full table
Discussion
Our study demonstrated that the high enhanced serosa sign on CT is associated with gastric cancer involvement of the serosa, probably owing to these causes. Gastric cancers are affected by diverse pathological factors such as cell differentiation, the amount of tissue stroma, the infiltration pattern, and the presence or absence of ulceration (15). Gastric cancers may thus show diverse findings on contrast-enhanced multidetector CT (MDCT).
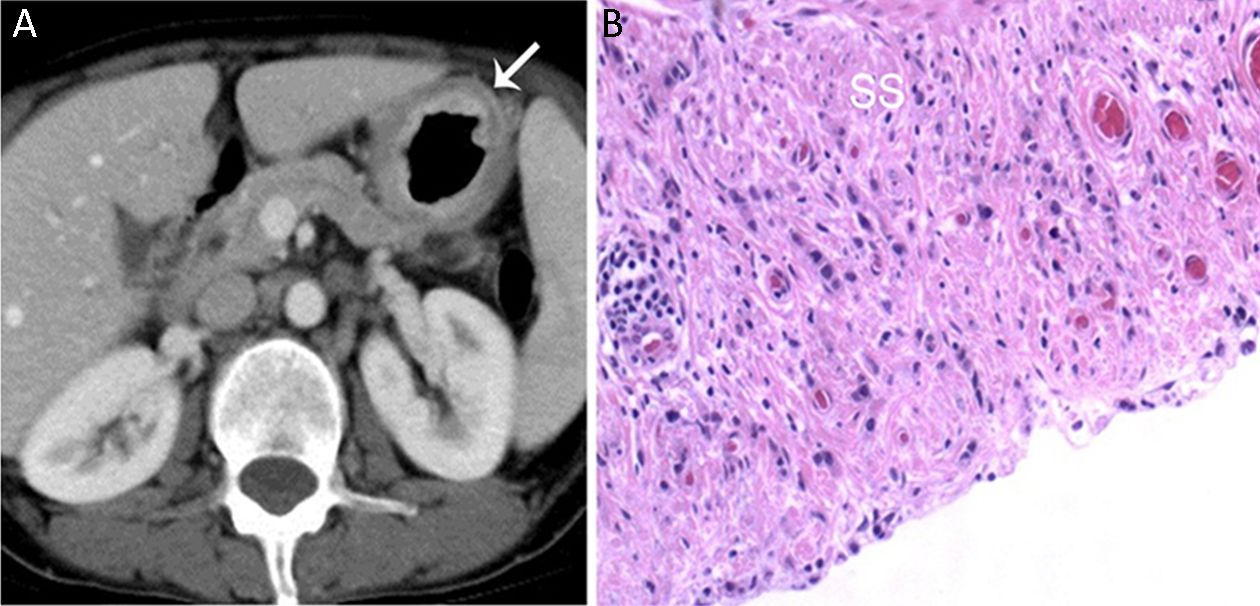
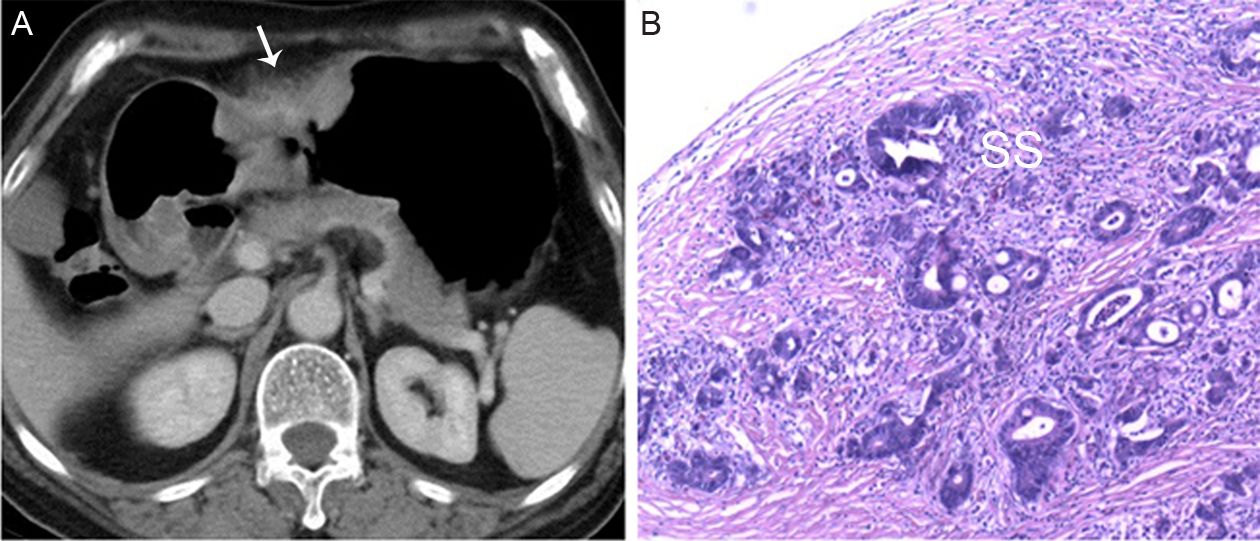
Our study also demonstrated that the sensitivity of the judgement of serosa invasion using the high enhanced serosa sign on CT in diffuse-type was significant higher than that in intestinal-type, some published studies of Lauren’s classification could explain this result (13-21). Pathologically, intestinal and diffuse gastric cancers differ in cellular cohesion, which is low in the diffuse-type (21). In diffuse gastric cancer, clusters of tumor cells infiltrate the gastric layers. Therefore, desmoplastic reaction and inflammatory peritumoral reaction are limited to the gastric wall, and a smooth and regular appearance of the outer surface is often seen (Figure 3). In intestinal gastric cancer, cells are more closely linked and organized in solid or glandular structures that replace the gastric layers completely. In these cases, desmoplastic and inflammatory reaction and necrosis produce a distortion of the outer gastric wall, which appears with reticular or linear soft-tissue density on CT images (Figure 4A), mimicking tumor invasion of the perigastric fat (21). The enhanced serosa was seen in intestinal gastric cancer (Figure 5), which manifested that the fibrosis strands and spiculations near the serosa could hardly distort the outer gastric wall. Therefore the hyperattenuating serosa was seen more specificly in intestinal-type than in diffuse-type. For the cases of mixed-type of gastric cancers, in which both intestinal and diffuse components were histologically shown, the features on CT were seen of both two types, which could explain the diagnostic performance of mixed-type did not show significant difference compared with other two types.

According to Lauren’s classification (10), two types of gastric cancer may be distinguished. The intestinal-type of gastric cancer is characterized by solid components and a glandular structure. Inflammatory cell infiltration due to host reaction occurs, concentrating especially at the margin of tumor spread (Figure 4B). This type of gastric cancer is associated with lymphatic or vascular invasion, and the lesions are scattered in distant positions (14). In diffuse gastric cancer, tumor cells lack adhesion and infiltrate the stroma as single cells or small subgroups, leading to a population of non-cohesive, scattered tumor cells. Cells seem to be scattered without forming distinct epithelial cords, with a high percentage of secreting cells and secreted mucus dispersed in the stroma (14,15,17). These tumors do not grow as a well-defined mass and have a wider spread inside the mucosa. Intestinal gastric cancer tends to spread locally, with vascular and other organ invasions. Whereas diffuse gastric cancer tends to spread more diffusely, with lymphatic invasion that can produce peritoneal seeding and ascites (20).
Histologically, a high-attenuating abnormal inner layer corresponded to where cancer cells were closely proliferated, mainly in the mucosal and submucosal layers, whereas a low-attenuating abnormal second layer corresponded to where cancer cells were diffusely scattered, mainly in the proper muscle layer with desmoplastic change and inflammatory reaction (17,18). In addition, the presence of a high-attenuating abnormal third layer on the serosal surface of the gastric wall suggested the serosal infiltration of the tumor because this high-attenuating layer histologically corresponded to a closely linked proliferation of cancer cells from the subserosal layer to the serosa, indicating direct serosal infiltration by the tumor (19).
Some new tools had been recently used to characterize gastric cancer, such as CT texture analysis, which analyses the distribution and relationship of pixel intensities in CT images, it might be able to reveal subtle differences that cannot be recognized by human eyes and to compensate for the shortage of conventional CT imaging. In addition, CT texture analysis provides an assessment of tumor heterogeneity at imaging and indirect information of tumor microenvironment with a range of quantified parameters.
Previous study concluded that the potential benefits of giving chemotherapy before surgery are the downsizing and downstaging of the primary tumor and lymph node metastases, treating micrometastases early in the course of treatment (22). Moreover, multimodal treatment of locally AGC provides reasonable 3-year survival compared with historical data (23).
Our study has excluded patients who underwent preoperative neoadjuvant therapy, which has been undertaken randomly in patients with AGCs in Peking University Cancer Hospital. Although in some clinical trials, neoadjuvant chemotherapy is more frequently used in the locally AGC with serosal invasion (22,23). Therefore, the selection of patients had little impact on the population bias.
Lauren classification exhibited a number of distinct clinical and molecular characteristics. Gastric cancer exhibits varied sensitivity to chemotherapy drugs and significant heterogeneity. Therefore, the Lauren classification may provide the basis for individualized treatment for AGC. T4a tumor penetrated the serosa and the potential rate of peritoneum metastasis was increased, which will lead to a poor prognosis. The analysis of CT features might help differentiate T3 from T4 gastric cancers, so that more timely selection of appropriate treatment strategies would be made.
Factors that could impact the analysis of CT images were as follows: 1) Gastric cancers with ulceration may be misdiagnosed in the depth of cancer invasion; 2) The lesions on the angular incisure of stomach, whose CT findings were not typical due to a collapsed gastric lumen; and 3) Cancers of the esophagogastric junction cannot be accurately analyzed because it may invade the gastric bare area without serosa coverage. That may explain why the overall sensitivity (Table 1) is low (63.7%–66.1%) in our study. For the T3 tumors whose paragastric inflammatory strands may mimic the cancer infiltration out of the serosa and lead to the overstaging, the high enhanced serosa sign is of important significance.
Our study has several limitations. First, the evaluation of the hyperattenuating serosa could be subjectively because the CT value of the stratified layers could not be measured precisely. Moreover, some of the CT images appear with reticular or linear soft-tissue density, which may mimic tumor invasion of the perigastric fat, this situation could be improved by the combination of new modalities [spectral CT, diffusion weighted magnetic resonance imaging (MRI), etc.]. Second, all of the cases in our series were resectable. It is unclear whether our results are applicable to unresectable gastric cancers. Third, the retrospective design of our study induced selection bias by limiting our study to patients with gastric cancer who underwent CT and surgery.
In addition, other imaging modalities were also proved of value in differentiation of staging. Several studies have confirmed the value of diffusion-weighted imaging (DWI) in detection (24) and characterization of gastric cancers. A characteristic appearance named “sandwich sign” can be widely and definitely observed on DW images, suggesting a stage ≥pT3 (25). MRI with DWI can increase the sensitivity and accuracy in TNM Classification of Malignant Tumors (TNM) staging of gastric cancers (26,27), especially in T staging (28).
Conclusions
The high enhanced serosa sign on CT is associated with gastric cancer involvement of the serosa. The sensitivity of the judgement of serosa invasion using hyperattenuating serosa sign in diffuse-type was significant higher than that in intestinal-type. The finding could be a key diagnostic feature for differentiating T3 from T4a stage gastric cancers.
Acknowledgements
This study has received funding by National Natural Science Foundation of China (No. 81471640, 81371715).
Footnote
Conflicts of Interest: The authors have no conflicts of interest to declare.
References
- Choi JK, Park YS, Jung DH, et al. Clinical relevance of the tumor location-modified Lauren classification system of gastric cancer. J Gastric Cancer 2015;15:183–90. [PubMed] DOI:10.5230/jgc.2015.15.3.183
- Tsurumaru D, Miyasaka M, Nishimuta Y, et al. Differentiation of early gastric cancer with ulceration and resectable advanced gastric cancer using multiphasic dynamic multidetector CT. Eur Radiol 2016;26:1330–7. [PubMed] DOI:10.1007/s00330-015-3938-2
- Hu B, El Hajj N, Sittler S, et al. Gastric cancer: Classification, histology and application of molecular pathology. J Gastrointest Oncol 2012;3:251–61. [PubMed] DOI:10.3978/j.issn.2078-6891.2012.021
- Li Z, Li Z, Jia S, et al. Depth of tumor invasion and tumor-occupied portions of stomach are predictive factors of intra-abdominal metastasis. Chin J Cancer Res 2017;29:109–17. [PubMed] DOI:10.21147/j.issn.1000-9604.2017.02.03
- Amin MB, Edge SB, Greene FL, et al. AJCC Cancer Staging Manual. 8th edition. New York: Springer, 2017.
- Washington K. 7th edition of the AJCC cancer staging manual: stomach. Ann Surg Oncol 2010;17:3077–9. [PubMed] DOI:10.1245/s10434-010-1362-z
- Giganti F, Ambrosi A, Chiari D, et al. Apparent diffusion coefficient by diffusion-weighted magnetic resonance imaging as a sole biomarker for staging and prognosis of gastric cancer. Chin J Cancer Res 2017;29:118–26. [PubMed] DOI:10.21147/j.issn.1000-9604.2017.02.04
- Kim JW, Shin SS, Heo SH, et al. Diagnostic performance of 64-section CT using CT gastrography in preoperative T staging of gastric cancer according to 7th edition of AJCC cancer staging manual. Eur Radiol 2012;22:654–62. [PubMed] DOI:10.1007/s00330-011-2283-3
- Kim TU, Kim S, Lee JW, et al. MDCT features in the differentiation of T4a gastric cancer from less-advanced gastric cancer: significance of the hyperattenuating serosa sign. Br J Radiol 2013;86:20130290. [PubMed] DOI:10.1259/bjr.20130290
- Lauren P. The two histological main types of gastric carcinoma: diffuse and so-called intestinal-type carcinoma. An attempt at a histoclinical classification. Acta Pathol Microbiol Scand 1965;64:31–49. [PubMed]
- Polkowski W, van Sandick JW, Offerhaus GJ, et al. Prognostic value of Laurén classification and c-erbB-2 oncogene overexpression in adenocarcinoma of the esophagus and gastroesophageal junction. Ann Surg Oncol 1999;6:290–7. [PubMed]
- Kim BS, Oh ST, Yook JH, et al. Signet ring cell type and other histologic types: differing clinical course and prognosis in T1 gastric cancer. Surgery 2014;155:1030–5. [PubMed] DOI:10.1016/j.surg.2013.08.016
- Flucke U, Mönig SP, Baldus SE, et al. Differences between biopsy- or specimen-related Laurén and World Health Organization classification in gastric cancer. World J Surg 2002;26:137–40. [PubMed] DOI:10.1007/s00268-002-0195-0
- Qiu MZ, Cai MY, Zhang DS, et al. Clinicopathological characteristics and prognostic analysis of Lauren classification in gastric adenocarcinoma in China. J Transl Med 2013;11:58. [PubMed] DOI:10.1186/1479-5876-11-58
- Ma J, Shen H, Kapesa L, et al. Lauren classification and individualized chemotherapy in gastric cance. Oncol Lett 2016;11:2959–64. [PubMed] DOI:10.3892/ol.2016.4337
- Park HK, Lee KY, Yoo MW, et al. Mixed carcinoma as an independent prognostic factor in submucosal invasive gastric carcinoma. J Korean Med Sci 2016;31:866–72. [PubMed] DOI:10.3346/jkms.2016.31.6.866
- Shimizu K, Ito K, Matsunaga N, et al. Diagnosis of gastric cancer with MDCT using the water-filling method and multiplanar reconstruction: CT-histologic correlation. Am J Roentgenol 2005;185:1152–8. [PubMed] DOI:10.2214/AJR.04.0651
- Chen YC, Fang WL, Wang RF, et al. Clinicopathological variation of Lauren classification in gastric cancer. Pathol Oncol Res 2016;22:197–202. [PubMed] DOI:10.1007/s12253-015-9996-6
- Hasegawa S, Yoshikawa T, Shirai J, et al. A prospective validation study to diagnose serosal invasion and nodal metastases of gastric cancer by multidetector-row CT. Ann Surg Oncol 2013;20:2016–22. [PubMed] DOI:10.1245/s10434-012-2817-1
- Esaki Y, Hirayama R, Hirokawa K. A comparison of patterns of metastasis in gastric cancer by histologic type and age. Cancer 1990;65:2086–90. [PubMed]
- Rossi M, Broglia L, Graziano P, et al. Local invasion of gastric cancer: CT findings and pathologic correlation using 5-mm incremental scanning, hypotonia, and water filling. Am J Roentgenol 1999;172:383–8. [PubMed] DOI:10.2214/ajr.172.2.9930788
- Ott K, Lordick F, Herrmann K, et al. The new credo: induction chemotherapy in locally advanced gastric cancer: consequences for surgical strategies. Gastric Cancer 2008;11:1–9. [PubMed] DOI:10.1007/s10120-007-0448-1
- Yoshikawa T, Sasako M, Yamamoto S, et al. Phase II study of neoadjuvant chemotherapy and extended surgery for locally advanced gastric cancer. Br J Surg 2009;96:1015–22. [PubMed] DOI:10.1002/bjs.6665
- Shinya S, Sasaki T, Nakagawa Y, et al. The usefulness of diffusion-weighted imaging (DWI) for the detection of gastric cancer. Hepatogastroenterology 2007;54:1378–81. [PubMed]
- Zhang XP, Tang L, Sun YS, et al. Sandwich sign of Borrmann type 4 gastric cancer on diffusion-weighted magnetic resonance imaging. Eur J Radiol 2012;81:2481–6. [PubMed] DOI:10.1016/j.ejrad.2011.10.021
- Caivano R, Rabasco P, Lotumolo A, et al. Gastric cancer: The role of diffusion weighted imaging in the preoperative staging. Cancer Invest 2014;32:184–90. [PubMed] DOI:10.3109/07357907.2014.896014
- Joo I, Lee JM, Kim JH, et al. Prospective comparison of 3T MRI with diffusion-weighted imaging and MDCT for the preoperative TNM staging of gastric cancer. J Magn Reson Imaging 2015;41:814–21. [PubMed] DOI:10.1002/jmri.24586
- Liu S, Wang H, Guan W, et al. Preoperative apparent diffusion coefficient value of gastric cancer by diffusion-weighted imaging: Correlations with postoperative TNM staging. J Magn Reson Imaging 2015;42:837–43. [PubMed] DOI:10.1002/jmri.24841